Elbow “TRASH” Lesions
CASE PRESENTATION
A 13-year-old male suffered a right elbow fracture dislocation from a fall (Figure 32-1A). He was treated by other orthopaedic surgeons with closed reduction and splint application emergently followed by a mobilization program (Figure 32-1B). He was referred 2 months postinjury due to lack of motion and concern about treatment for a developing elbow contracture. His arc of elbow flexion-extension was 30 to 100 degrees with slight crepitus. Neurovascular status was normal.
CLINICAL QUESTIONS
What does the acronym “TRASH” lesion mean?
What does “muffled crepitus” on physical exam indicate?
What is the significance of an elbow dislocation in a child less than 10 years of age?
What is the role of ultrasound in the evaluation of elbow trauma?
When is an MRI scan indicated with elbow trauma?
How useful are intraoperative arthrograms?
How aggressive should we be surgically in displaced osteochondral injuries in young children?
What are the reconstructive options for late-presenting osteochondral malunions?
THE FUNDAMENTALS
Etiology and Epidemiology
Osteochondral fractures and subtle radiographic elbow bone and joint malalignment can be missed by the best of clinicians. The minimal bony ossification in the first 5 years of life (only the capitellum and radial head) and the vagaries and limits of ossification between years 5 and 10 of life (see Sidebar) make plain radiographic diagnosis of some elbow fracture dislocations difficult. Missing these injuries acutely can result in a disastrous elbow functional outcome. Late reconstruction offers more complex challenges yet with more limited surgical options than acute treatment. Thus, the statement, “The Radiographic Appearance Seemed Harmless” yielded the term TRASH lesion.1 These lesions are mostly osteochondral fractures in children less than age 10 years.2, 3, 4, 5 and 6 You have to be meticulous in your clinical and radiographic analysis at all times with elbow region injuries and utilize ultrasounds, arthrograms, and magnectic resonance imaging (MRI) scans as diagnostic aids when in doubt.7,8
Clinical Evaluation
With TRASH lesions, the history of the trauma (fall off a second-story porch) and/or the degree of elbow region swelling often do not match the radiographic appearance. The lack of ossification in the elbow just does not give you enough information to connect all the dots in order to make the right diagnosis. It is a trap you want to avoid. So, start with the exam. Anytime you have massive swelling and what you think is a pretty normal x-ray, think again. Do not mistake a small fleck of bone as a minor injury. Do not think that a minimal joint malalignment is a minor issue. To paraphrase Dr. John Hall, “TRASH lesions are not like throwing horseshoes. Being close does not count.”
If there is restricted, painful motion, or specifically “muffled crepitus” (displaced, unstable cartilage moving against cartilage or bone) with elbow motion, you have to be worried. You need more imaging to find the answer. And, if the injury story does not match the degree of swelling in a very young child, you need to be very concerned about nonaccidental trauma and obtain appropriate scanning radiographs, bone scans, and pediatric and social service consultation.
The specific injuries include (1) transphyseal fractures before capitellar ossification (Figure 32-3) (see Chapter 27); (2) anterior compression fractures of the cartilaginous radial head that lead to posterior radial head subluxation (Figure 32-4); (3) displaced medial condylar fractures before the secondary center of ossification appears (Figure 32-4) (see Chapter 29); (4) plastic deformation Monteggia lesions (see Chapter 30); (5) intra-articular osteochondral elbow fractures (olecranon, radial head, capitellum, trochlea); (6) entrapped medial
epicondylar fractures4, 5 and 6 (Figure 32-5) (see Chapter 29); (7) lateral condylar and epicondylar osteochondral avulsions that represent an unstable lateral collateral ligamentous injury (Figure 32-6); (8) complex osteochondral fracture dislocations with multiple intra-articular fractures; and (9) an elbow dislocation at <10 years of age should make you nervous for multiple sites of injury not always readily apparent on plain radiographs.
epicondylar fractures4, 5 and 6 (Figure 32-5) (see Chapter 29); (7) lateral condylar and epicondylar osteochondral avulsions that represent an unstable lateral collateral ligamentous injury (Figure 32-6); (8) complex osteochondral fracture dislocations with multiple intra-articular fractures; and (9) an elbow dislocation at <10 years of age should make you nervous for multiple sites of injury not always readily apparent on plain radiographs.
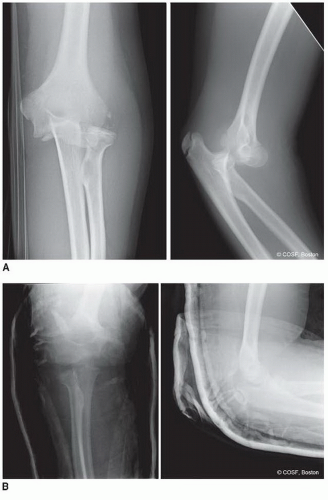 FIGURE 32-1 A: Radiographs of an elbow dislocation with lateral bony fragments. B: Closed reduction radiographs in splint. Note on the lateral view that the joint is not anatomic. |
Further radiographic evaluation is warranted with these rare injuries.7,8 You have to know that danger is lurking around the corner. Your referring team of pediatricians, emergency room caregivers, radiologists, and trainees need to be aware of the possibility of missing something important on plain radiographs of the elbow in a young child. Oblique views of the affected elbow and comparison views of the contralateral elbow might be helpful in proper diagnosis or even just increasing your suspicions that something is not right. Ultrasounds have been shown to be helpful with skilled hands (technical part) and eyes (interpretive part). For some clinicians, ultrasounds are mere confusion, and for others, they bring clarity. If you look at a lot of hip ultrasounds for dysplasia, the elbow ultrasound will make more sense to you. The use of MRI scans is extremely helpful for most surgeons, as the MRI images match the anatomy we are used to seeing and on which we base our decisions. Arthrograms are also helpful and used most often in the operating room as a part of both diagnosis and treatment (see Chapter 28, Sidebar). Very good clinicians have missed a TRASH injury and regretted it. Obtaining one or more of these additional radiographic studies acutely, or as a part of an evaluation of a chronic condition, is important for prompt, precise treatment. You
need to know exactly what the problem is before you can make the right decisions on fixing it.
need to know exactly what the problem is before you can make the right decisions on fixing it.
SIDEBAR
Secondary Centers of Ossification about the Elbow
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


