Injuries to the shoulder in pediatric and adolescent athletes are increasingly being seen with expanded participation and higher competitive levels of youth sports. Injury patterns are unique to the growing musculoskeletal system and specific to the demands of the involved sport (1, 2, 3, 4). Recognition of injury patterns with early activity modification and the initiation of efficacious treatment can prevent disability and return the youth athlete to sport. This chapter reviews the diagnosis and management of common shoulder injuries in the pediatric athlete.
DEVELOPMENTAL ANATOMY AND GROWTH
The shoulder complex involves four articulations and multiple ossification centers. Growth occurs through the cartilaginous physis. Bony development occurs through the primary and secondary centers of ossification and through periosteal bone formation. The cartilaginous physis is particularly vulnerable to acute macrotraumatic and repetitive microtraumatic injury (5).
Prenatally, the limb buds develop during the fourth gestational week (1, 2, 3, 4). The central core of the humerus appears as a cartilaginous anlage and the clavicle begins to ossify through intramembranous ossification by the fifth week. The scapula also appears around this time and is positioned proximally at the level of C4-5. The precursor to the shoulder joint, the interzone, also appears between the humerus and scapula. During the sixth gestational week, the hand begins to develop, bone formation occurs in the primary center of ossification of the humerus, and the interzone develops a layered configuration with a chondrified layer on either side of a loose layer of central cells. In the seventh week, the upper limbs rotate laterally, the shoulder joint is formed, and the scapula descends to its position between the first and fifth ribs. The muscular, tendinous, and ligamentous structures of the shoulder become distinct by the 13th gestational week and continue to mature throughout the gestational period.
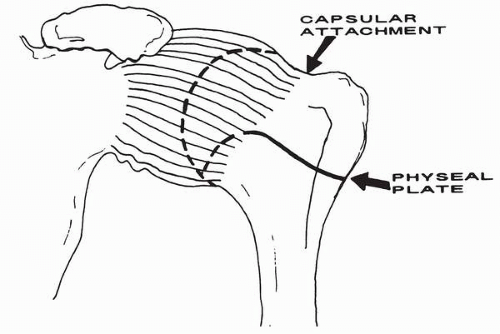
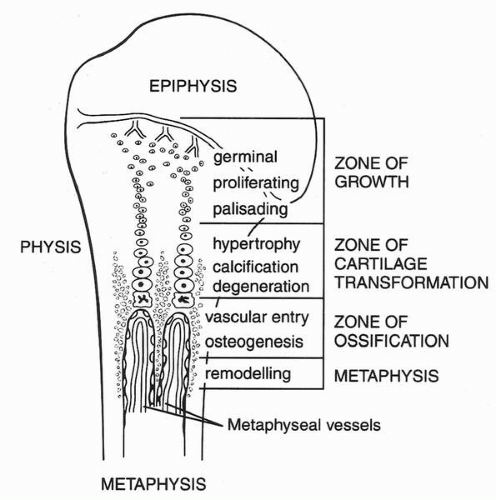
The secondary center of ossification of the proximal humeral epiphysis is usually seen after 6 months of age. Additional ossification centers appear at the greater tuberosity between 7 months and 3 years of age and at the lesser tuberosity is seen 2 years later. By age 5 to 7 years, these centers coalesce to form the proximal humeral epiphysis. The proximal humeral physis is extraarticular, except medially where the capsule extends beyond the anatomic neck, inserting on the medial metaphysis (Fig. 20-1). The proximal humeral physis contributes approximately 80% of the longitudinal growth of the humerus and usually fuses between 19 and 22 years of age. Fractures of the proximal humeral physis often occur through the zone of hypertrophy (Fig. 20-2).
The clavicle forms by intramembranous ossification. The medial secondary ossification center appears between 12 and 19 years of age and does not fuse to the shaft until age 22 to 25 years. The lateral epiphysis is inconstant, appearing, ossifying, and fusing over a period of a few months at about age 19 years.
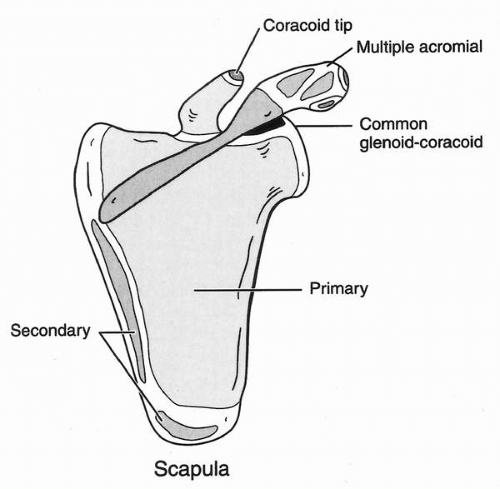
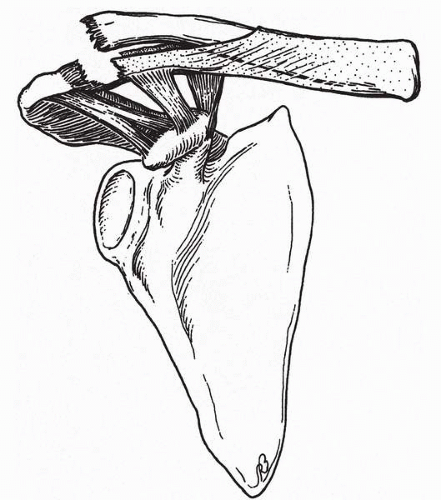
The scapula appears as a cartilaginous anlage in the first gestational week at the C4-5 level and gradually descends to its adult-like position overlying the first to fifth ribs. Failure to descend results in persistent elevation of the scapula and limited glenohumeral motion (Sprengel’s deformity). The scapula ossifies via intramembranous ossification with multiple remaining secondary ossification centers (Fig. 20-3). The ossification center of the coracoid process appears at approximately 1 year of age, coalescing with the ossification center of the upper glenoid by age 10 years. The acromion ossifies by multiple (2, 3, 4, 5) ossification centers which usually appear about puberty and fuse by age 22 years. Failure of fusion of one of these ossification centers may result in an os acromiale. Various other scapular malformations may occur, including bipartite coracoid, acromion duplication, glenoid dysplasia, and scapular clefts. In the first 2 years of life, the glenoid is retroverted approximately 6 degrees, but reaches adult retroversion of 2 to 6 degrees by the end of the first decade of life.
FIGURE 20-1. Proximal humeral physis and glenohumeral joint capsule. The physis is mostly extraarticular except medially. (From Curtis RJ. Anatomy, biomechanics, and kinesiology of the chil ‘s shoulder. In: DeLee JC, Drez D, Miller MD, eds. Orthopaedic sports medicine: principles and practice, 2nd ed. Philadelphia: WB Saunders, 2003, with permission.)
FIGURE 20-2. Proximal humeral physis. Fractures often occur through the zone of hypertrophy. (From Curtis RJ. Anatomy, biomechanics, and kinesiology of the child’s shoulder. In: DeLee JC, Drez D, Miller MD, eds. Orthopaedic sports medicine: principles and practice, 2nd ed. Philadelphia: WB Saunders, 2003, with permission.)
FIGURE 20-3. Ossification centers of the scapula. (From Curtis RJ. Anatomy, biomechanics, and kinesiology of the child’s shoulder. In: DeLee JC, Drez D, Miller MD, eds. Orthopaedic sports medicine: principles and practice, 2nd ed. Philadelphia: WB Saunders, 2003, with permission.)
Maturation and Laxity
In addition to longitudinal growth of the upper and lower extremities, the pediatric athlete is developing in terms of maturation (1, 2, 3, 4). The child’s stage of maturation is often an important factor in injury patterns. In addition, girls mature at an earlier age than boys. Less mature children often have less muscular development and may be in a period of rapid longitudinal growth, predisposing to repetitive overuse injuries. More mature children may have increased muscular development and less longitudinal growth remaining, leading to acute, macrotraumatic injuries. The Tanner staging system is usually used to classify children with respect to secondary sexual development and maturation (Table 20-1).
During childhood and adolescence, changes in laxity also occur. Laxity is common in younger children and less common through adolescence. In newborns, type III collagen is synthesized, and the fibers formed from type III collagen are supple and elastic. With each passing decade, collagen-producing cells make less type III collagen and progressively convert to making type I collagen, which is more nonelastic. This changing ratio of type I and III collagen is so reliable that the chronologic age of an individual can be determined by analyzing the type III collagen of a skin sample (6). Some patients, particularly girls, may exhibit generalized ligamentous laxity of multiple joints (7, 8, 9). Because of the importance of capsuloligamentous restraints for shoulder stability, patients with laxity may experience difficulty with glenohumeral instability.
TABLE 20-1. TANNER STAGING CLASSIFICATION OF SECONDARY SEXUAL CHARACTERISTICS
Tanner Stage
Male
Female
Stage 1 (prepubertal)
Growth
5-6 cm/yr
5-6 cm/yr
Development
Testes <4 mL or <2.5 cm
No breast development
No pubic hair
No pubic hair
Stage 2
Growth
5-6 cm/yr
7-8 cm/yr
Development
Testes 4 mL or 2.5-3.2 cm
Breast buds
Minimal pubic hair at base of penis
Minimal pubic hair on labia
Stage 3
Growth
7-8 cm/yr
8 cm/yr
Development
Testes 12 mL or 3.6 cm
Elevation of breast; areolae enlarge
Pubic hair over pubis
Pubic hair of mons pubis
Voice changes
Axillary hair
Muscle mass increases
Acne
Stage 4
Growth
10 cm/yr
7 cm/yr
Development
Testes 4.1-4.5 cm
Areolae enlarge
Pubic hair as adult
Pubic hair as adult
Axillary hair
Acne
Stage 5
Growth
No growth
No growth
Development
Testes as adult
Adult breast contour
Pubic hair as adult
Pubic hair as adult
Facial hair as adult
Mature physique
Other
Peak height velocity: 13.5 years
Adrenarche: 6-8 years
Menarche: 12.7 years
Peak height velocity: 11.5 years
EPIDEMIOLOGY AND INJURY PATTERNS
Injuries to the pediatric athlete’s shoulder are being seen with increased frequency. There has been increased participation in youth sports (10). In addition, children are participating in organized athletics at higher competitive levels with increased intensity. It is not uncommon to see a youth pitcher with a sore shoulder who plays in two concurrent leagues, throws a large number of pitches during games and practices, and who has been taught split finger pitches. Less than 10% of the 2.5 million volunteer coaches and less than one third of the interscholastic coaches in the United States have had any type of coaching education. The sequelae of these injuries are of importance. Sports injuries to youth ages 0 to 14 years for 29 sports in 1997 cost the U.S. public nearly $50 billion according to the U.S. Consumer Product Safety Commission (11). In addition, injuries to youth athletes can result in permanent disability and deformity.
Injury patterns to the pediatric athlete’s shoulder tend to be sport specific. In football, the shoulder ranks second only to the knee in number of overall injuries (12, 13, 14). These injuries tend to result from macrotrauma, such as glenohumeral dislocation, acromioclavicular separation, and clavicle fractures. Bicycling is a popular recreational and sporting activity among children and adolescents. Sixty percent of all bicycle injuries occur in children between the ages of 5 and 14 years and 85% of injuries involve the upper extremity (10,15). A common injury pattern during bicycling involves lateral clavicle fracture or acromioclavicular separation from landing on the point of the shoulder when thrown from the bicycle. Shoulder injuries during alpine skiing and snowboarding are being seen with increased frequency and account for approximately 40% of upper extremity injuries and 10% of all injuries (16,17). Thirty percent of wrestling injuries occur in the upper extremity, with the shoulder being the most commonly involved location. Injury to the acromioclavicular joint is frequent, resulting from a direct blow of the shoulder against the mat (18).
The pediatric shoulder is particularly vulnerable in overhead athletes. In baseball, injury to the pediatric shoulder from throwing is a result of microtrauma from repetitive motions of large rotational forces (19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35). The proximal humeral physis is particularly vulnerable to these large, repetitive forces, resulting in a chronic physeal stress fracture (Little League shoulder) (36, 37, 38, 39, 40, 41, 42, 43, 44, 45). The shoulder in tennis is similarly subjected to repetitive overhead motions involving large torques. Impingement and depression of the shoulder (tennis shoulder) may result (46). Repetitive microtrauma also frequently leads to shoulder dysfunction in swimmers (47). The risk of injury is related to competitive level and event type. Injuries include impingement syndrome and glenohumeral instability. Multidirectional instability is often seen and is related to the underlying ligamentous laxity often seen in swimmers. Similarly, multidirectional instability can be seen in gymnasts who also frequently demonstrate generalized ligamentous laxity. Additional shoulder injuries unique to gymnasts include cortical hypertrophy at the pectoralis major insertion (ringman’s shoulder) and supraspinatus tendinitis (48, 49, 50, 51, 52, 53, 54).
SPECIFIC INJURIES
Sternoclavicular Joint Injury
True sternoclavicular joint dislocations are rare in the skeletally immature. The characteristic injury involves a physeal fracture of the medial clavicle, commonly a Salter-Harris I or II injury, in that the medial clavicular physis does not fuse until the early 20s (55, 56, 57, 58, 59, 60). The epiphysis stays attached to the sternum via the stout sternoclavicular ligaments and the medial clavicular shaft displaces posteriorly or anteriorly. Medial clavicular injury often results from an indirect force transmitted along the clavicle from a direct blow during contact sports to the lateral shoulder. If the shoulder is driven forward, posterior displacement of the medial clavicle occurs. Conversely, if the shoulder is driven posteriorly, anterior displacement of the medial clavicle occurs.
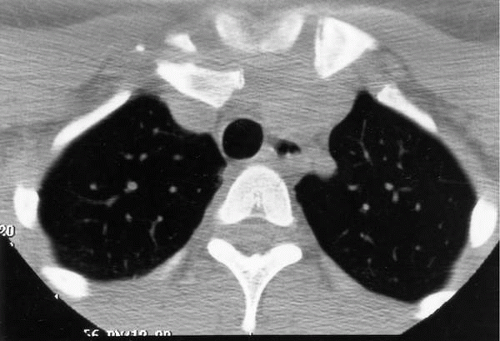
The patient often describes a pop in the region of the sternoclavicular joint and there is tenderness to palpation of the medial clavicle. The direction of displacement may be obscured by marked swelling. Posterior displacement can be a medical emergency because the medial clavicle can impinge on vital mediastinal structures including the innominate great vessels, trachea, and esophagus (Fig. 20-4). Venous congestion, diminished pulses, dysphagia, or dyspnea should alert the clinician to the possibility of such injury. Standard anteroposterior (AP) radiographs of the chest or sternoclavicular joint are often hard to interpret given the overlapping spinal, thoracic, and mediastinal structures. A tangential radiograph obtained in a 40-degree cephalad-directed manner (the serendipity view) may aid in visualization of the medial clavicle displacement. Definitive delineation of the fracture pattern and direction of displacement is provided by computed tomography scan.
FIGURE 20-4. Sternoclavicular joint injury. Axial computed tomography scan demonstrating physeal fracture/separation of the medial clavicle with compression of the innominate vein in a 16-year-old female.
Minimally displaced fractures heal readily. Attempted reduction of anteriorly displaced fractures can be accomplished under local anesthesia or sedation by placing the patient supine with a bolster between the scapulae. The arm is abducted 90 degrees and then extended with gentle posterior pressure directly over the medial clavicle followed by protraction of the shoulder. After reduction, the shoulder is immobilized in a figure-of-eight dressing or shoulder immobilizer and gentle range of motion exercises are started as pain allows. Most fractures heal in 3 to 4 weeks and return to sport requires full painless range of motion and strength. Unstable fractures usually heal and remodel rapidly. Posteriorly displaced medial clavicular fractures with impingement of mediastinal structures require emergent reduction with thoracic surgery standby for the rare but potential injury of the major thoracic vessels. Under general anesthesia with the patient supine, traction is applied to the arm with the shoulder extended, and a towel clip can be used to reduce the medial clavicle. There is little indication for open reduction and internal fixation of medial clavicular physeal fractures, and catastrophic complications of pin migration from hardware about the sternoclavicular joint has been reported. On rare occasion, open reduction with stabilization may be indicated for patients with recurrent, symptomatic instability. In younger children, repair of the torn periosteum is usually sufficient for stability, whereas older children and adolescents require reconstruction of the medial sternoclavicular ligamentous structures using palmaris tendon or semitendinosus tendon graft.
Clavicle Fracture
The clavicular shaft is vulnerable to injury from direct blows during contact sports. In addition, indirect forces on the outstretched arm may lead to clavicular fracture. The clavicular shaft is mechanically vulnerable as a strut given its S-shaped configuration and the strong ligamentous bindings at either end. With fracture, there is limited shoulder motion and tenderness over the fracture site, and the skin overlying the fracture may be tented and compromised. The proximal fragment may be elevated superiorly due to spasm of the sternocleidomastoid or trapezius muscles. Significant neurovascular injury is rare but should be assessed clinically given the proximity of the subclavian vessels and the brachial plexus. Radiographs are usually sufficient for diagnosis and management. Younger children may exhibit a greenstick fracture or plastic deformation.
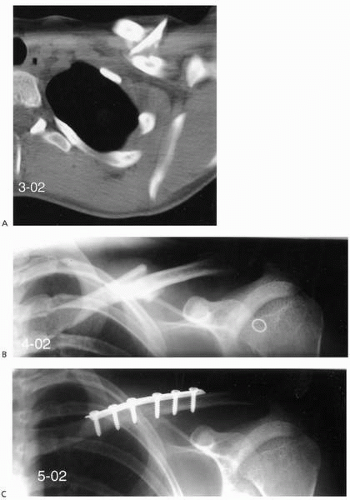
The prognosis of most clavicular shaft fractures in children is excellent (61, 62, 63). Immobilization is accomplished by a figure-of-eight bandage or shoulder immobilizer. Slings that exert significant pressure to effect a reduction should be avoided. Even displaced fractures usually heal readily with a bump of healing callus that remodels over a period of 6 to 12 months. Return to sport is allowed when the clavicle is nontender, there is radiographic union, and motion and strength are full. This usually occurs by 4 to 6 weeks in younger children and by 6 to 10 weeks in the adolescent. Significant malunion that does not remodel and nonunion of clavicular shaft fractures in the skeletally immature are rare. Malunion with a symptomatic bump can be treated after healing with osteoplasty. Open reduction and internal fixation is indicated for open fractures, fractures with significant neurovascular compromise, threatened skin from fracture displacement (Fig. 20-5), and floating shoulder injuries.
FIGURE 20-5. Clavicle fracture. A comminuted clavicle fracture in a 14-year-old female athlete. A: Computed tomography scan demonstrates the comminuted fragment tenting the skin. Preoperative (B) and postoperative (C) radiographs obtained after open reduction and internal fixation.
Acromioclavicular Joint Injury
A fall on the point of the shoulder usually results in acromioclavicular separation in the adult and older adolescent, but results in physeal fracture of the lateral clavicle in children (63, 64, 65, 66, 67, 68, 69, 70, 71). With lateral clavicle fracture and true acromioclavicular separation in the pediatric patient, displacement of the lateral clavicle occurs superiorly through a tear in the thick periosteal tube surrounding the distal clavicle (Fig. 20-6). The lateral clavicular epiphysis along with the acromioclavicular and coracoclavicular ligaments usually remain intact to the periosteal tube.
The pediatric athlete with lateral clavicle physeal fracture or acromioclavicular injury usually presents after a fall or contact to the point of the shoulder. Pain and deformity are localized to the acromioclavicular joint. Plane radiographs are usually sufficient to evaluate the injury and stress radiographs with 5 to 10 pounds of traction may aid in delineating the degree of instability. An axillary lateral view demonstrates AP displacement. Like for adult acromioclavicular injuries, Rockwood has classified pediatric acromioclavicular injuries based on the position of the lateral clavicle and the accompanying injury to the periosteal tube (71). Type I injuries involve mild sprain of the acromioclavicular ligaments without disruption of the periosteal tube. Type II injuries involve partial disruption of the dorsal periosteal tube with slight widening of the acromioclavicular joint. Type III injuries involve a large dorsal disruption of the periosteal tube with gross instability of the distal clavicle. Type IV injuries involve disruption of the periosteal tube with posterior displacement of the lateral clavicle (Fig. 20-7). Type V injuries involve periosteal tube disruption with greater than 100% superior subcutaneous displacement of the lateral clavicle. Type VI injuries involve an inferior subcoracoid dislocation of the lateral clavicle.
FIGURE 20-6. Acromioclavicular injury. Displacement of the distal clavicle occurs through a tear in the periosteal tube of the clavicle. The acromioclavicular and sternoclavicular ligaments remain intact to the periosteal tube. (From Beim GM, Warner JP. Clinical and radiographic evaluation of the acromioclavicular joint. Oper Tech Sports Med 1997;5:68, with permission.)
Nonoperative management of acromioclavicular injuries in children younger than 13 years old is the mainstay of treatment because these injuries usually represent a physeal fracture rather than a true acromioclavicular joint dislocation (63, 64, 65, 66, 67, 68, 69, 70, 71). Thus, these injuries exhibit a great potential for healing and remodeling because the periosteal tube usually remains in continuity with the epiphyseal fragment and acromioclavicular and coracoclavicular ligaments. For type IV, V, and VI injuries with very large displacement, operative stabilization may be indicated. Repair of the periosteal tube with or without internal fixation is usually performed. For late adolescent and adult-type true acromioclavicular joint separations, nonoperative management results in good outcomes for type I and II injuries, whereas operative management is indicated for type IV, V, and VI injuries. The management of type III injuries in the older adolescent athlete remains controversial, as with adults, with many recommending initial nonoperative management (64,68,69).
Osteolysis of the Distal Clavicle
Osteolysis of the distal clavicle is an overuse injury resulting from repetitive microtrauma (72). It has also been described as a sequela following traumatic injury to the distal clavicle or acromioclavicular joint; however it is seen most commonly in adult weightlifters. In addition, this entity is being identified in other sports since cross-training has become more popular and in younger athletes who are weight training year-round for higher level sports. Patients complain of an aching discomfort about the acromioclavicular joint after workouts, with the pain progressing to interfere with training and eventually with activities of daily living. There is tenderness to palpation of the distal clavicle and pain with cross-chest adduction. Treatment consists of rest, particularly from weight training, and antiinflammatory medications. For those who fail conservative treatment or who are unable to refrain from weight training, distal clavicle resection usually results in resolution of pain and return to sport.
Little League Shoulder
As a result of repetitive microtrauma from the large rotational torques involved in throwing, chronic stress fracture of the proximal humeral physis can occur (19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35). This entity has been termed Little League shoulder and is most commonly seen in high-performance male pitchers between 12 and 14 years old (36, 37, 38, 39, 40, 41, 42, 43, 44, 45). The rotator cuff muscles attach proximal to the proximal humeral physis, whereas the pectoralis major, deltoid, and triceps muscles attach distally. In addition to age and the large rotational forces of pitching, poor throwing mechanics and frequent pitching may predispose to injury. In an extensive study of Little League pitchers, Albright found that those who had poor pitching skills were more likely to be symptomatic (20).
Only gold members can continue reading. Log In or Register to continue