CHAPTER 7 Diagnostic Shoulder Arthroscopy and Bursoscopy
PREOPERATIVE CONSIDERATIONS
Snyder1 has emphasized the importance of performing a complete 15-point glenohumeral examination and an 8-point bursoscopy examination in every arthroscopic shoulder procedure. Doing so will improve a surgeon’s arthroscopic skills in not only maneuvering the arthroscope, but also in diagnosing and treating almost all disorders of the shoulder joint arthroscopically.
ARTHROSCOPIC TECHNIQUE
In recent years, many advances have been made in shoulder arthroscopy, and we are now capable of performing complex arthroscopic shoulder procedures that were once deemed impossible. However, attention to detail is paramount, and this begins with the setup of the patient and the operating room. Every arthroscopic shoulder procedure requires careful preoperative and operative planning. The shoulder arthroscopist should always have a full complement of instruments available at all times, including cannulas, anchors, and suturing devices. The possibility of an arthrotomy should be discussed in advance with the patient in the event that pathology requiring an open approach is encountered. At the time of diagnostic arthroscopy, unexpected pathology can be found that may need to be addressed; it should not be ignored simply because the surgeon and staff did not have the proper instrumentation available or an adequate consent form signed.
Patient Positioning and Setup
Diagnostic shoulder arthroscopy and bursoscopy can be performed with the patient in the beach chair or lateral decubitus position. We prefer the lateral decubitus position using a commercially available arm supporter. The device is attached to the opposite side of the operating table via the Clark rail of the table. It is then rotated toward the operative shoulder. The arm is draped using a U-drape around the neck running distally and a 10-10 drape across the chest anterior to posterior. This draping is important because it prevents fluid extravasation onto the chest wall or neck. The entire extremity is prepped from the fingertips to the neck and axilla. A sterile shoulder sleeve is then affixed to the arm. The arm is supported by attaching the triangle at the end of the sleeve to the overhead cable ring using the sterile S hook (Fig. 7-1A). Ten pounds of weight using balanced suspension is attached to the upper cable for the average-sized person, but a few pounds more or less may be needed for larger or smaller limbs.1 The suspension device is color-coded so that the surgeon can advise the circulating nurse where to place the weight in an effort to abduct the shoulder for entrance into the glenohumeral joint or adduct the shoulder to facilitate entry into the subacromial space.
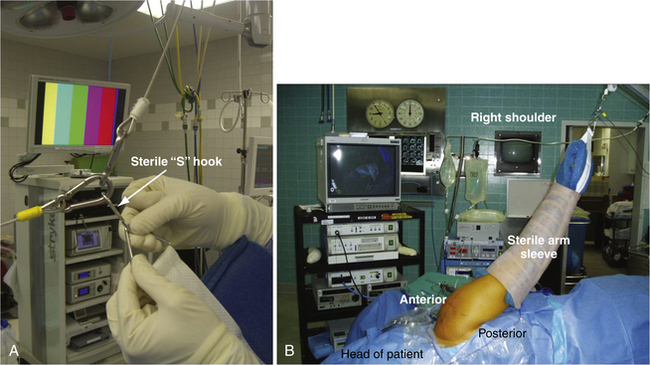
For diagnostic glenohumeral shoulder arthroscopy in the lateral decubitus position, the arm is positioned in 70 degrees of abduction and 15 to 20 degrees of forward flexion (see Fig. 7-1B). The surgeon stands behind the patient and the assistant is usually at the head of the table. If there is a second assistant or scrub tech, he or she stands behind the two surgeons. The drapes are allowed to drop over the head of the patient and the anesthesiologist can be at the head of the patient. The tubes and monitoring devices are stretched far enough so that the surgeon can walk around the head of the patient to the front to work anteriorly. All equipment is in front of the surgeon, including the video monitor, shaver, pump, and suction, with all tubes running off a Mayo stand on the other side of the patient. This prevents tangling of the multiple cords and tubing used in shoulder arthroscopy and also allows the surgeon easy and quick visibility of all equipment to ensure that everything is working properly during the procedure.
Use of a Trained Assistant
In private practice, or even in an academic setting, it is important to build your surgical team. Most shoulder arthroscopy is performed as an outpatient procedure and many are done in an outpatient surgery center. A surgical scrub technician can be trained to be a valuable first assistant for shoulder arthroscopy. By working together every week, operating room personnel learn your routine and the many steps involved in complex arthroscopic shoulder cases. Instructing them to hold the arthroscope properly allows the surgeon to use two hands to perform anchor placement, knot tying, and other parts of the arthroscopic procedure.
Surface Anatomy
With the arm supported in suspension, outlining the surface anatomy with a sterile marking pen is the next step before making any skin incisions. The supraclavicular fossa is first outlined; it is bordered anteriorly by the clavicle and acromioclavicular (AC) joint, laterally by the acromion, and posteriorly by the spine of the scapula. Next, the most outer or inferior edges of the clavicle, acromion, and spine of the scapula are palpated and dots are used as reference points (Fig. 7-2A). Connect the dots to define the most lateral acromial border, the S-shaped anterior edge of the clavicle, and the scapular spine posteriorly (see Fig. 7-2B). By palpating the most lateral aspect of the supraclavicular fossa, the AC joint is located at a 45-degree angle anteriorly (see Fig. 7-2C).
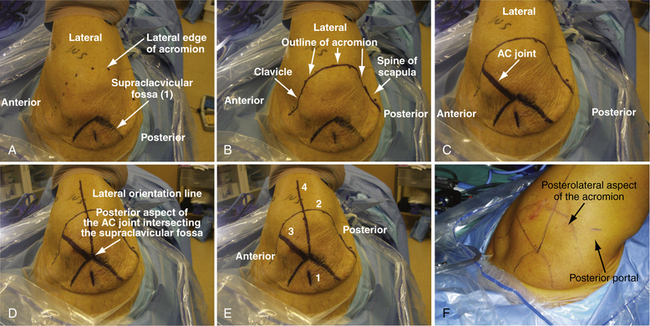
The lateral orientation line is drawn next. At the posterior aspect of the AC joint (i.e., the anterior edge of the supraclavicular fossa, where it intersects the AC joint), a line is drawn out laterally that crosses perpendicular to the lateral border of the acromion and extends distally 4 cm down the arm. This reference line divides the acromion into an anterior two fifths and posterior three fifths (see Fig. 7-2D and E). The orientation line is helpful as a reference when creating the lateral subacromial portal for decompression and arthroscopic rotator cuff repair procedures.1
Posterior and Anterizor Portal Creation
The first step in performing an arthroscopic evaluation of the glenohumeral joint is to create the posterior superior portal and to introduce the posterior cannula. In an average-sized individual, the entry point is approximately 2 cm inferior and 1cm medial from the posterolateral acromial edge (see Fig. 7-2F). For patients with thicker tissue or larger bony structures, the point is further inferior and medial.1 A 1-cm or smaller incision is made through the skin only with a no. 11 blade. The arthroscopic metal cannula with a blunt-tipped obturator is inserted through the posterior skin incision through the muscle until the posterior humeral head is palpated. With the opposite hand palpating the anterior surface of the shoulder joint, the humeral head is gently rotated back and forth. The opposite hand, which is placed anteriorly over the coracoid, should feel the movement of the humeral head. This also allows one to localize the joint line. The cannula is then directed medially and slightly inferior (raising your hand slightly) to slide medially off the humeral head. Aiming toward the coracoid process can be helpful in orientation when establishing this portal. Working the cannula through the capsule, one usually feels a definite popping sensation as the joint is entered. The arthroscope should then be placed into the cannula after the obturator is removed to verify placement and avoid multiple holes in the posterior capsule with repetitive attempts, which could lead to increased fluid extravasation.
A common error in making the posterior superior portal is to make it too lateral or proximal. The joint line is located inferior and medial to the posterolateral acromial corner.1 If difficulties are encountered in entering the glenohumeral joint, especially in larger patients, it is helpful to place 5 more pounds of suspension (total, 15 pounds). This provides more distraction and it is easier to palpate the step-off between the humeral head and glenoid with the tip of the blunt obturator. Never use excessive pressure or a sharp trocar in the cannula because penetration of the humeral head or scraping and damaging the articular surface can occur. After the capsule is punctured, the arthroscope is inserted to ensure that the cannula is truly in the joint and not in the subacromial space.1 If an extra 5 pounds of suspension had been added, removal at this time helps avoid inadvertent neurovascular compromise.
When the arthroscope is inserted into the posterior cannula, the joint is distended with an arthroscopic pump. The pump pressure is set between 30 to 60 mm Hg to maintain optimal visualization. The minimum pressure is maintained and adjusted frequently to control bleeding. The biceps tendon is visualized and the anterior portal can be created using an inside-out or outside-in technique. If an outside-in technique is used, a spinal needle is first placed to localize the portal (Fig. 7-3A) and the portal is created.
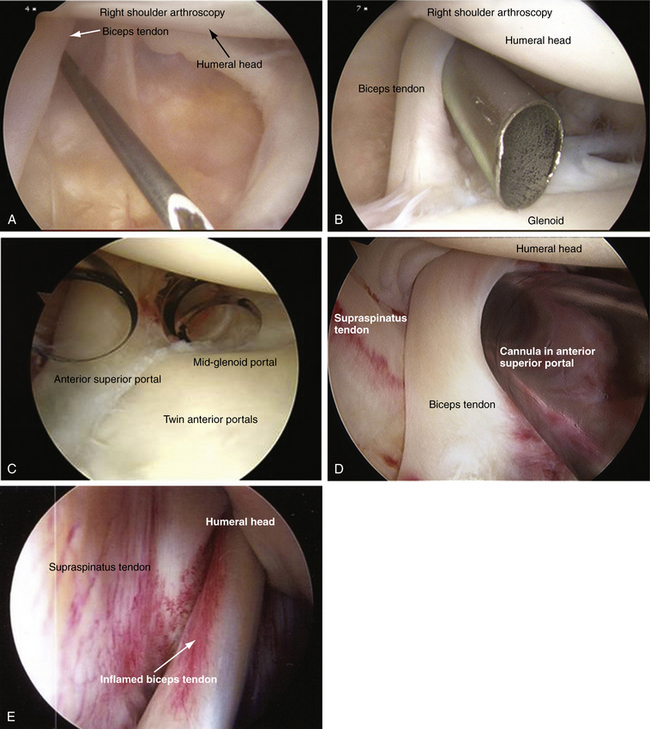
We prefer using an inside-out technique because it is quick, easy, and reproducible. The arthroscope is gently driven across the glenoid, just below the biceps tendon, and into the rotator interval. The arthroscope is removed and a blunt, smooth switching stick is inserted through the cannula, tenting the skin anteriorly. This requires little force and, if significant resistance is met, the switching stick may have migrated too superiorly into the supraspinatus tendon. A small stab incision is made at the tip of the rod and the rod is passed through the skin incision. A metal or plastic cannula is then inserted over the guide rod and gently twisted in until the capsule is penetrated. Using a metal cannula makes it easier to penetrate the anterior capsule and also is interchangeable so that the arthroscope can be easily switched from posterior to anterior during the diagnostic arthroscopy (see Fig. 7-3B).
The anterior portal is created in an anterior -superior position in the rotator interval between the anterior edge of the supraspinatus and the subscapularis tendons. By creating the portal superiorly, superior labrum anterior posterior (SLAP) pathology can be addressed as the angle for inserting a superior glenoid anchor is facilitated. This location also ensures a suitable viewing portal for evaluating anterior labral anatomy and pathology. It also ensures that there is adequate space for a second anterior midglenoid working portal, which can be created at the leading edge of the subscapularis tendon (see Fig. 7-3C).
Diagnostic Arthroscopy of the Glenohumeral Joint
With the patient in the beach chair or lateral decubitus position, a complete glenohumeral examination can be performed. The importance of a systematic 15-point glenohumeral diagnostic arthroscopy1 cannot be overemphasized and we recommend that it be performed during every shoulder arthroscopy. Proper arthroscopic handling, with rotation of the bevel of the arthroscope, allows systematic joint visualization. By rotating the arthroscope and using the angle of the arthroscopic lens to the surgeon’s advantage, it is possible to obtain a greater visual field without actually changing the position of the arthroscope within the joint. Nowhere is this more important than in the shoulder, where looking around the corner is a necessary skill. For this discussion, all the following arthroscopic manipulation positions described pertain to a right shoulder.
Position 1
The first structure to be viewed in a systematic 15-point glenohumeral examination is the biceps tendon, followed by the superior labrum.1 For a right shoulder, the arthroscope is positioned with the 30-degree angle looking up at 11 o’clock. This allows the biceps to be visualized (see Fig. 7-3D) and, using the anterior cannula as a probe, the biceps can be pulled into the joint for inspection. Inflammation (see Fig. 7-3E) or partial tears of the biceps tendon can be hidden in the extra-articular portion or within the intertrabecular groove and may not be not readily visualized.
Rare variants of the biceps tendon, including a partial or conjoined tendon, complete intra-capsular position, or absence of the tendon, may be encountered.2 A double structure (bifid) of the long head of the biceps tendon has been reported.3 The vincula biceps can occasionally be seen; these are small strands of mesentery-like synovium that pass from the biceps tendon to the surrounding synovium and capsule. On occasion, if robust enough, the vinculae can prevent retraction of a torn proximal biceps.1
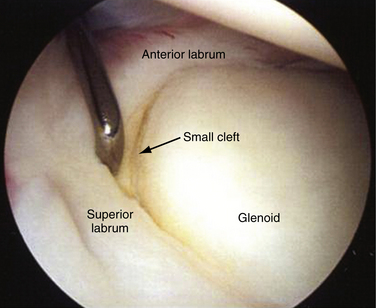
The 30-degree bevel of the arthroscope is then rotated down to about the 8 o’clock position and the superior labrum is visualized. Again, using the edge of the cannula as a probe, the superior labrum can be palpated at its attachment to the superior glenoid. Stoller4 has described three different types of attachment for the biceps labral complex (BLC) to the glenoid. A type 1 BLC is firmly attached to the superior glenoid, with no sublateral foramen in the anterosuperior quadrant. A probe can be inserted through the anterior superior portal to palpate the labrum (Fig. 7-4). A type 2 BLC is attached several millimeters medial to the sagittal plane of the glenoid, and articular cartilage continues to coat the superior aspect of the glenoid surface underneath the labrum. A small cleft between the glenoid and labrum is not uncommon. In a type 3 BLC, the labrum is meniscoid in shape, loosely attached, and exhibits a large sulcus that projects under the labrum and over the cartilaginous pole of the glenoid. This should not be confused with a type II SLAP tear. Traction on a normal biceps tendon should not produce arching or detachment of the labrum away from the superior glenoid.1
A degenerative superior labrum (type I SLAP) is also normal and can be débrided, but does not treatment (Fig. 7-5A). A type II SLAP tear demonstrates granulation tissue between the glenoid and superior labrum, and is best visualized when a probe retracts the damaged labrum (see Fig. 7-5B). A type III SLAP lesion is a split of the superior labrum (see Fig. 7-5C) whereas a type IV SLAP lesion represents a split that extends into the biceps and may be fragmented (see Fig. 7-5D).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


