Development of the Foot and Ankle
Shahan K. Sarrafian
Armen S. Kelikian
PRENATAL DEVELOPMENT
The embryonic period is divided into 23 horizons or stages. Each horizon corresponds to a developmental stage of the embryo based on a system of point scores. This method of classification and identification of the embryo advocated by Streeter has brought greater precision to embryologic descriptions.1 Embryos of different crown-rump (C-R) lengths might belong to the same horizon. The growth curve of the embryo, correlating the C-R length with the fertilization or menstrual age of the embryo, as presented by Patten (Fig. 1.1), is used throughout this study.2 The use of a growth curve in terms of one linear measurement correlated with age is still of value for the interpretation of embryologic information predating Streeter’s classification.
Morphogenesis of the Feet
Morphogenesis of the feet is illustrated in Figures 1.2 and 1.3.1 The embryo of 2 weeks post fertilization is curved irregularly in a semicircle and presents no external evidence of a lower limb bud in the caudal area (Fig. 1.4).
Horizons or Stages of Development
At 3 weeks, a slight longitudinal swelling is discernible opposite the five lumbar and first sacral myotomes. Once initiated, the ontogeny of the lower limb progresses in a rapid sequential fashion, and definite morphologic changes are recognizable at 2-day intervals. At 4 weeks, in horizon 13 (3 to 6 mm), a minute lower limb bud germinates at the site of the previous swelling. Within the next 2 days, in horizon 14 (5 to 7 mm), the bud increases in size and springs laterally from the trunk. It exhibits a flat ventral and a rounded dorsal surface united by a convex margin (see Figs. 1.2 and 1.5). In horizon 15 (6 to 9 mm), the bud extends its base distally toward the sacral myotomes and further increases in length. The lumbar segment retains a round contour, whereas the sacral part tapers. A differentiation is initiated and is well evident in horizon 16 (8 to 11 mm). Three regions are visible, corresponding to the thigh, the leg, and the foot anlage. All three regions are more or less located in the same transverse plane, which is perpendicular to the plane of the lower trunk.
A rounded foot disk is recognized in horizon 17 (11 to 13.5 mm) at the fifth embryonic week. The surface of the foot plate is located in the transverse plane, and the ventral surface, the future plantar surface, faces the head. An inward rotation occurs, and the future flexor surface obliquely faces the median sagittal plane of the trunk (see Figs. 1.2 and 1.6). When viewed from the ventral aspect of the embryo, the rotation of the foot plate—a fundamental change—is counterclockwise on the left and clockwise on the right; the leg segment participates in this inward rotation. Morphologically, no toe rays are present in the foot plate. However, older embryos of this group have an indication of the great toe on the tibial or preaxial border. Within the next 2 days, in horizon 18 (14 to 16 mm; see Fig. 1.2), the sixth embryonic week, the inward rotation of the foot-leg segment continues. The medial surface of the foot plate faces more toward the median plane of the trunk, and this surface, when extended distally, makes with its counterpart an acute angle, open proximally. When the embryo is viewed from the lateral aspect, the future dorsal surface of the foot plate can be seen. An inward rotation of nearly 90 degrees has occurred. The preaxial or tibial border is cephalad, and the postaxial or peroneal border is caudad. Digital rays are clearly visible, and some interdigital notching is present. In horizon 19 (16.5 to 20 mm), the features of the previous stage are accentuated. The digital notching is deeper (see
Figs. 1.2 and 1.7). The foot plates are converted to a more recognizable foot structure in horizon 20 (21 to 23 mm; see Figs. 1.3 and 1.8), and by horizon 21 (22 to 24 mm; see Fig. 1.3), the seventh embryonic week, the orientation of the parts is as follows:
Figs. 1.2 and 1.7). The foot plates are converted to a more recognizable foot structure in horizon 20 (21 to 23 mm; see Figs. 1.3 and 1.8), and by horizon 21 (22 to 24 mm; see Fig. 1.3), the seventh embryonic week, the orientation of the parts is as follows:
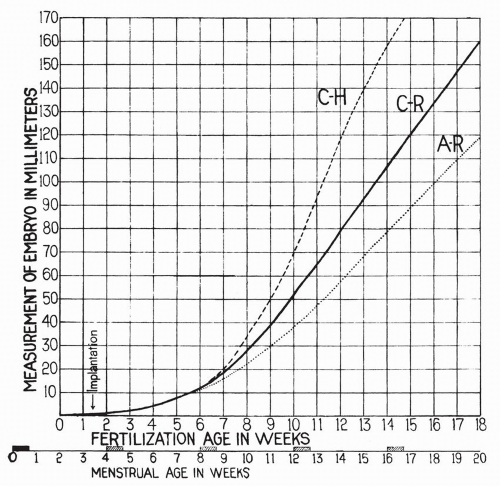 Figure 1.1 Crown-to-rump (C-R) length as compared with age of embryo. (After Patten BM. Human Embryology. 2nd ed. New York: McGraw-Hill; 1953:185.) |
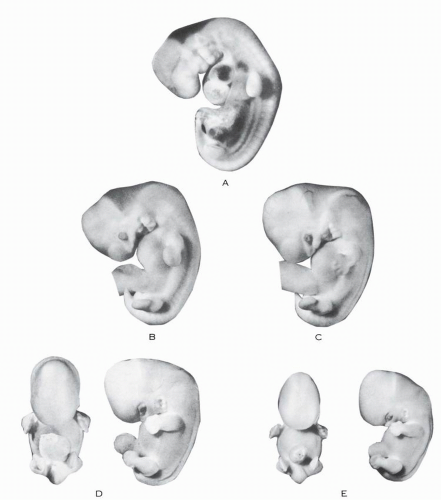 Figure 1.2 Embryos. (A) Horizon 14 (4.9 to 8.2 mm). (B) Horizon 16 (8 to 11 mm). (C) Horizon 17 (11 to 13.5 mm). (D) Horizon 18 (14 to 16 mm). (E) Horizon 19 (16.5 to 20 mm). (Assembled after Streeter GL. Developmental horizons in human embryos. Contrib Embryol. 1945, 1948, 1951; 21, 32, 34.) |
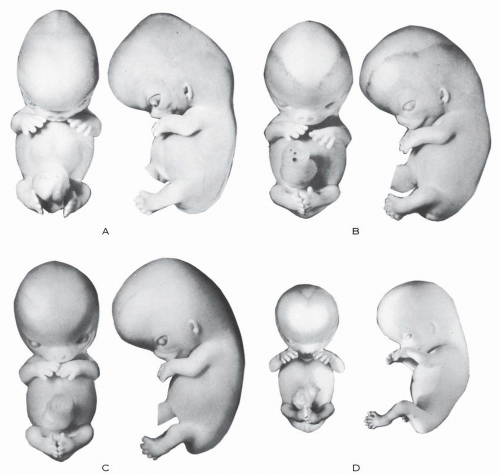 Figure 1.3 Embryos. (A) Horizon 20 (21 to 23 mm). (B) Horizon 21 (21 to 24 mm). (C) Horizon 22 (25 to 27 mm). (D) Horizon 23 (28 to 30 mm). (Assembled after Streeter GL. Developmental horizons in human embryos. Contrib Embryol. 1945, 1948, 1951; 21, 32, 34.) |
Both feet face each other and are located in a nearly sagittal plane.
The preaxial or tibial border of the leg-foot is cephalad.
The postaxial or fibular border of the leg-foot is caudad.
The extensor surface (future anterior surface of the leg and dorsum of the foot) faces laterally.
The flexor surface (future posterior surface of the leg and plantar of the foot) faces medially.
The toes are well delineated and spread apart. The big toe is on the tibial border of the foot.
The foot surface is in continuity with the leg surface.
There is no dorsal angulation of the foot relative to the leg.
The foot is in an equinus position relative to the leg.
The entire lower extremity is in a position of marked external rotation.
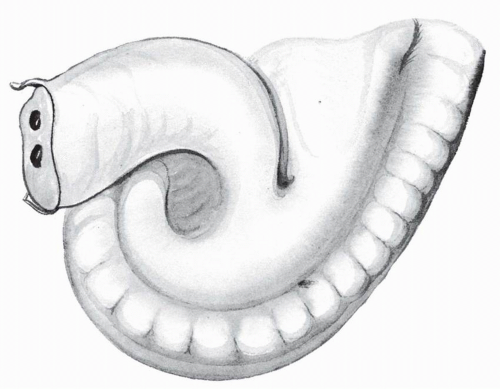 Figure 1.4 Embryo of 4.2 mm. |
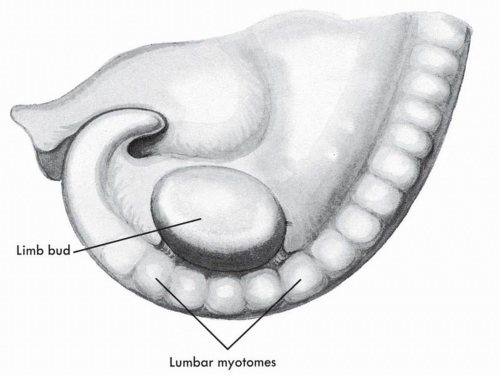 Figure 1.5 Embryo of horizon 14 (6.3 mm). |
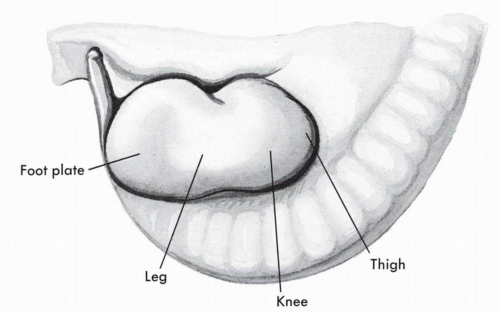 Figure 1.6 Embryo of horizon 17 (11 to 13.5 mm). |
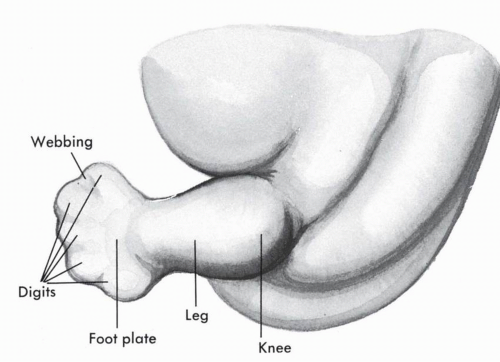 Figure 1.7 Embryo of horizon 19 (17.5 mm). |
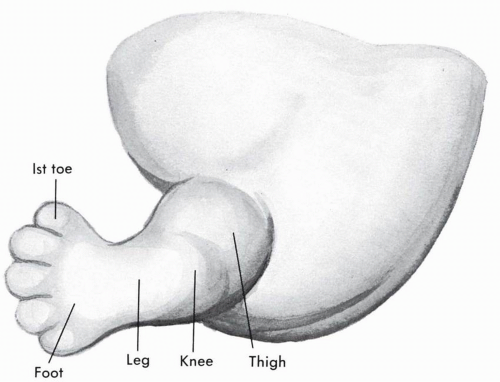 Figure 1.8 Embryo of horizon 20 (20 mm). |
Horizon 23 marks the end of the embryonic period proper (see Figs. 1.3 and 1.9). It corresponds to the end of the eighth embryonic week and an average C-R length of 30 mm. The feet touch each other at their soles or medial aspects and are in a praying position. The toes are still fanning out.
During the fetal period, important rotational changes take place that alter the leg-foot relationship. Initially the feet, their soles facing each other, are in equinus relative to the leg. A progressive internal rotation of the thigh-leg occurs, and the foot is then in equinus, supination, and external rotation relative to the leg. Subsequently, the foot dorsiflexes and pronates, bringing the foot close to the adult neutral position; the toes do not diverge.
Böhm, describing the developmental phases of the foot in the embryo-fetus, ascribes four stages to the morphologic determinism.3
Stage one (second month): The foot is in 90-degree equinus and adducted.
Stage two (beginning of third month): The foot is in 90-degree equinus, adducted, and markedly supinated.
Stage three (middle of third month): The foot dorsiflexes at the ankle, but a mild degree of equinus is still present. The marked supination persists. The first metatarsal remains adducted. This stage corresponds to the fetal period of development.
Stage four (beginning of fourth month): The foot pronates and reaches a position of midsupination. A slight metatarsus varus remains. The equinus is not present.
The pronation “continues during the remainder of foetal development and is not yet complete in the newborn.”3
The division of the development of the foot into four stages brings schematic clarity, but in reality, as Böhm states, “the changes do not actually occur within the exact limits of four stages, but by means of gradual, continuous transformations.”3
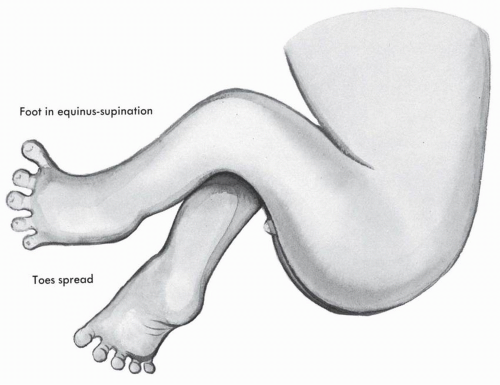 Figure 1.9 Embryo of horizon 23 (28 to 33 mm). |
Digital Formula
The study of the position and relative length of the toes presents another interesting aspect of the morphogenesis of the foot (Fig. 1.10).
The pedal digits make their clear appearance in horizon 20 (21 to 23 mm). They diverge from the convex border of the foot plate. The third toe arises from the apex of the convexity and is therefore the longest. Within a few days, the preaxial side of the foot grows more rapidly, and the second toe surpasses the third.4 It is later in fetal life that the first toe might take the lead. According to Jones, in the very early embryo, the pedal digit formula may be 3 >2>1>4>5 or 3>2>4>1>5 for a brief period.4 When the embryo reaches horizon 22 (25 to 27 mm), the second toe takes the lead with a 2>3>1>4>5 distribution; later, the adult formula is reached in the form of 1>2>3>4>5 or its variant 2>1>3>4>5.
I have analyzed the pedal digital formula in 29 embryo feet. The feet were classified according to length into three developmental groups: group 1, feet up to 5 mm in length; group 2, feet 5 to 9 mm in length; group 3, feet 10 mm in length. The following distribution was present:
Group 1 (5 feet total):
Four feet (3 mm, 4 mm, 4 mm, 4.5 mm): 3>2>4>1>5
One foot (4 mm): 2>3>4>1>5
Group 2 (19 feet total):
One foot (5.5 mm): 3>4>2>1>5
Seven feet (5 mm, 5.5 mm, 5.5 mm, 6 mm, 6 mm, 6 mm, 6 mm): 3>2>4>1>5
Six feet (6 mm, 6 mm, 6 mm, 7 mm, 8 mm, 8 mm): 2>3>4>1>5
Four feet (5 mm, 6.5 mm, 7 mm, 9.5 mm): 2>3>1>4>5
One foot (8 mm): 2>1>3>4>5
Group 3 (5 feet total):
2 feet (11 mm, 12 mm): 2>1>3>4>5
One foot (10 mm): 2>3>1>4>5
Two feet (11 mm, 14 mm): 1>2>3>4>5
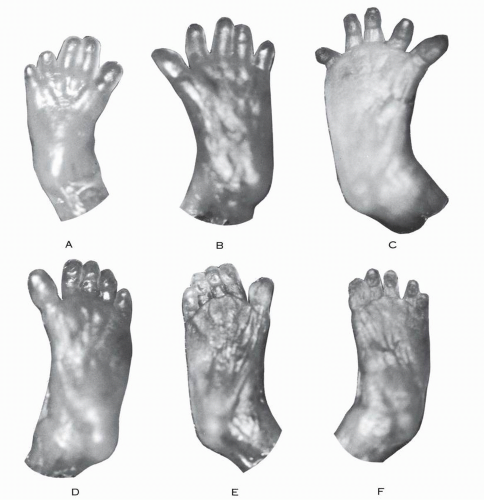 Figure 1.10 Feet of embryos. Length: (A) 3.5 mm; (B) 4 mm; (C) 5.5 mm; (D) 5 mm; (E) 6 mm; and (F) 6 mm. |
It is apparent, based on these measurements, that the third toe is the longest in the very young embryo. As the embryo grows, the third toe loses its place to the second. Later, the first toe moves next to the second, thus reaching one variation of the adult digital formula (2>1>3>4>5), and in the oldest embryos of this group (11 and 14 mm) the first toe took the lead with the common adult distribution (1>2>3>4>5).
Metatarsal Formula
In the embryo, the metatarsal formula initially is 3>2>1>4>5 or 3>2>4>5>1. In the fourth and fifth month of fetal life, the rule is 2>3 >1>4>5, already resembling the common adult formula. From the sixth to the ninth month, the metatarsal formula is 2>1>3>4>5 or the occasional variant 2>3>1>4>5.5
Plantar or Walking Pads
Plantar or walking pads are soft-tissue elevations produced by localized accumulation of subcutaneous connective tissue and fat (Fig. 1.11).6
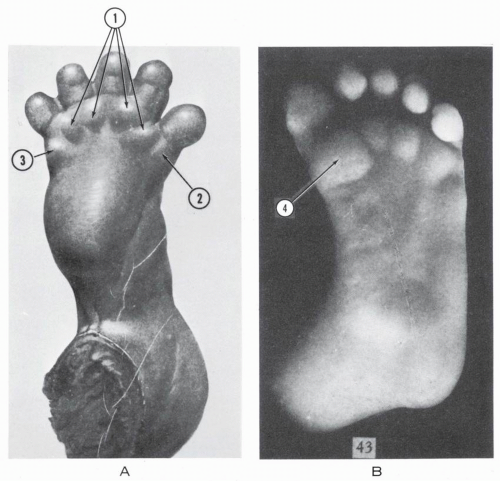 Figure 1.11 Plantar pads. (A) Foot of 24-mm embryo (1, interdigital pads; 2, tibial pad; 3, fibular pad). (B) Foot of 62.5-mm embryo (4, hallucal pad formed by fusion of tibial pad and first interdigital pad). (After Cummins H. The topographic history of the volar pads [walking pads, tastballen] in the human embryo. Contrib Embryol. 1929;20:105.) |
In the embryo of horizon 20, four distal plantar pads appear, corresponding to the interdigital spaces. A tibial pad and a fibular pad are also separately indicated. The proximal region of the sole of the foot shows no distinct pads. By horizon 22, five apical pads appear on the plantar aspect of the toes distally. The distal interdigital pads become more prominent in horizon 23, and on the tibial side the first interdigital pad and the tibial pad merge to form the “hallucal pad.” The interdigital pads are reduced to three. A central sole pad now makes its appearance, and the heel region is also slightly elevated. In the embryo of 40 mm, the central pad is nearly level. A general regression of the pads occurs when the fetus is 100 mm in C-R length or older. The pads become gradually lower and discrete. These pads persist during the remaining period of gestation in discrete regressed form.
In the last fetal weeks, the feet are swollen and the pads are temporarily masked. In the postnatal phase, the hallucal and interdigital pads are demonstrable, and the fibular pads are not noticeable.
Foot Growth
Foot measurement is possible only after the embryo reaches a C-R length of 24 mm, that is, after horizon 21.7, 8
In the early fetal stage (30 to 60 mm), the foot grows less rapidly than the body (sitting height). After 70 mm, until term,
there is retardation in the increase of sitting height, whereas the foot maintains its growth rate and displays a relative acceleration of growth. This increase in foot length is slow from the 8th to the 14th week, then becomes more rapid until the 26th week, then slows down slightly until term. The average increase in length from the 14th week on is about 3 mm per week, with only slight variation.7 The tabulated data of Scammon and Calkins, when converted into a growth curve, give the pattern shown in Figure 1.12.8 At the end of the third month, the foot measures on average 0.8 cm and at term the average length is 7.6 cm (maximum, 8.7 cm; minimum, 7.1 cm). These dimensions are measured as a straight line from the posterior margin of the heel to the tip of the extended big toe.
there is retardation in the increase of sitting height, whereas the foot maintains its growth rate and displays a relative acceleration of growth. This increase in foot length is slow from the 8th to the 14th week, then becomes more rapid until the 26th week, then slows down slightly until term. The average increase in length from the 14th week on is about 3 mm per week, with only slight variation.7 The tabulated data of Scammon and Calkins, when converted into a growth curve, give the pattern shown in Figure 1.12.8 At the end of the third month, the foot measures on average 0.8 cm and at term the average length is 7.6 cm (maximum, 8.7 cm; minimum, 7.1 cm). These dimensions are measured as a straight line from the posterior margin of the heel to the tip of the extended big toe.
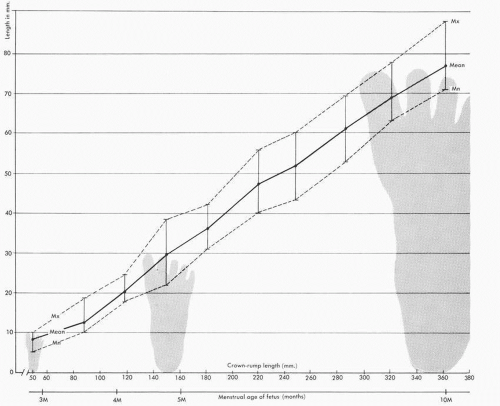 Figure 1.12 Prenatal foot growth and length. (Curves based on data from Scammon RE, Calkings LA. The Development and Growth of the External Dimensions of the Human Body in the Fetal Period. Minneapolis: University of Minnesota Press; 1929:245-246.) |
The fetal foot narrows gradually with growth and remains longer than the adult foot when compared with the corresponding tibia length. The ratio of greatest foot length/tibia length is 1.41 at 8 weeks, 0.9 at birth, and 0.6 in the adult.5
Internal Structures
Skeleton
The lower limb bud makes its appearance in horizon 13 (3 to 6 mm) at 4 weeks post fertilization. The bud is filled with blastemic tissue. An ectodermal thickening forms on the ventral aspect, and within 4 days (horizon 15) it is converted into an
ectodermal ridge on its lateral part. This ridge is transient and disappears within a week (horizon 19). Its importance seems primordial, because it induces the differentiation of the future limb components and determines their directional (proximodistal) formation.9
ectodermal ridge on its lateral part. This ridge is transient and disappears within a week (horizon 19). Its importance seems primordial, because it induces the differentiation of the future limb components and determines their directional (proximodistal) formation.9
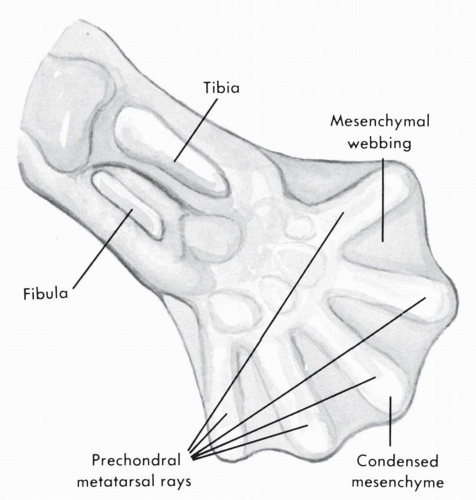 Figure 1.13 Foot plate of embryo in horizon 18 (14 to 16 mm). Skeleton in mesenchymal stage. (After Bardeen CR. Studies of the development of the human skeleton. Am J Anat. 1905;4:265.) |
Stages of Skeletal Development
There are three stages in the formation of skeletal elements: mesenchymal, cartilaginous, and osseous.
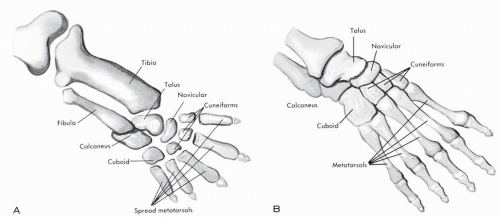 Figure 1.14 (A) Foot and leg of embryo in horizon 19 (20 mm). Skeleton in cartilaginous stage. (B) Foot and ankle of 33-mm fetus. Skeleton in cartilaginous stage. (After Bardeen CR. Studies of the development of the human skeleton. Am J Anat. 1905;4:265.) |
Mesenchymal. The mesenchymal stage is illustrated in Figure 1.13.10, 11 In horizons 17 (11 to 13 mm) and 18 (14 to 16 mm), the foot plate is already present. The axial mesenchyme condenses, differentiates, and forms the anlage of the foot. The metatarsals differentiate later. When the phalangeal models are formed, for a short time a thick web remains between the digital rays. The metatarsal rays are spread apart, but they will gradually approximate.
The differentiation of the tarsus follows that of the metatarsals. Within the areas of condensation tissue, procartilage soon makes its appearance. The lower ends of the tibia and fibula are still formed of condensed blastemic tissue in horizon 20.
Cartilaginous. The cartilaginous stage is illustrated in Figure 1.14. Cartilage cells form in the mesenchymal-prochondral anlage. As the process of chondrification advances, the skeletal elements become clearly identifiable; morphogenesis, aiming toward the adult form, occurs. The chronologic sequence of chondrification was reported by Senior.12 The process occurs in 14 stages (Fig. 1.15). The central three metatarsals chondrify first, followed by the fifth metatarsal and the cuboid. The chondrification of the tarsus continues with the calcaneus, the talus, and the third and second cuneiforms. The first cuneiform and the first metatarsal follow. The navicular is the last tarsal element to chondrify. The phalanges are next, and the process occurs in a proximodistal sequence.
The proximal phalanges of the second, third, and fourth toes chondrify, followed by the proximal phalanx of the fifth toe. The proximal phalanx of the big toe is next, to be followed by the middle phalanges of central toes two, three, and four. Next in sequence is the chondrification of the middle phalanx of the
little toe, the distal phalanx of the big toe, and the distal phalanges of the second, third, and fourth toes. The last element to chondrify is the distal phalanx of the little toe.
little toe, the distal phalanx of the big toe, and the distal phalanges of the second, third, and fourth toes. The last element to chondrify is the distal phalanx of the little toe.
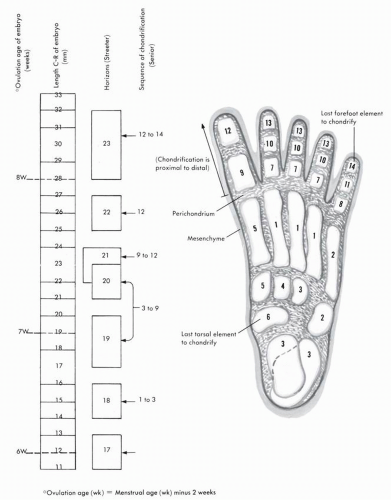 Figure 1.15 Chronologic sequence of chondrification of the foot in the embryo. (Based on data from Senior HD. The chondrification of the human hand and foot skeleton [abstr]. Anat Rec. 1929;42:35. Correlation between sequence of chondrification and Streeter’s horizons based on O’Rahilly R, Gray DJ, and Gardner E. Chondrification in the hands and feet of staged human embryos. Contrib Embryol. 1957;36:185.) |
The chondrification of the foot is initiated in horizon 18 (14 to 16 mm), and the last element, except for the sesamoids, chondrifies in horizon 23 (28 to 32 mm), which represents the end of the embryonic period proper.
The relationship between Senior’s sequence of chondrification and Streeter’s horizons (see Fig. 1.15) has been reported by O’Rahilly and coworkers.11
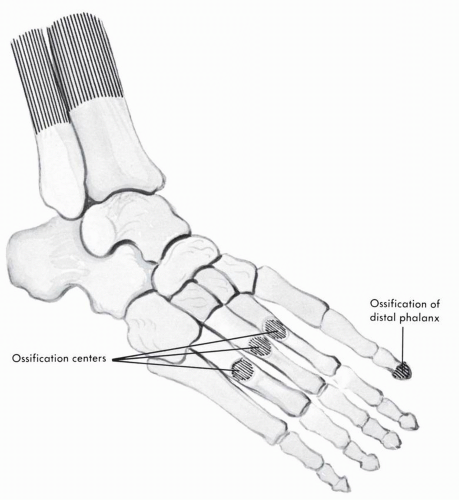 Figure 1.16 Foot of 50-mm fetus. Skeleton at onset of ossification. (After Bardeen CR. Studies of the development of the human skeleton. Am J Anat. 1905;4:265.) |
Within a given condensed mesenchymal unit, chondrification of the future anatomic components occurs at different times. The body of the calcaneus begins to chondrify centrally in horizon 18, the tuber calcanei in horizon 21, and the sustentaculum tali in horizon 23.13
By the end of the embryologic period proper, the morphology and relationship of the cartilaginous skeletal components are determined and resemble closely those of the adult. The future articular surfaces acquire their definite contour at this early stage, prior to the formation of a joint space.10
Chondrification is present in the distal tibia and fibula in horizon 21.
Osseous. The osseous stage is shown in Figures 1.16 and 1.17.10, 13, 14 The forefoot ossifies before the hindfoot. The general sequence of ossification is distal phalanx of the big toe, metatarsals, distal phalanges of lesser toes, proximal phalanges, and finally middle phalanges. The last element to ossify in the forefoot is the middle phalanx of the little toe. The ossification of the forefoot takes place between the third and fifth prenatal lunar months.
In the hindfoot, the calcaneus is the first to ossify. Gardner and associates describe periosteal bone formation on the inferolateral aspect of the calcaneus in a 93-mm fetus.13 At 125 mm, the endochondral center of ossification appears. The talus may begin to ossify during the eighth lunar month, but an ossification center is not always present at birth. An extensive study correlating roentgenographic findings with body weight in the newborn indicates that regardless of the weight of the newborn, the calcaneus is always ossified; the talus is also ossified except in infants weighing less than 2000 g.15 In this low-birth-weight group, talar ossification was absent at birth in an average of 13.3% of infants. The cuboid is the last tarsal element that can exhibit prenatal ossification.
The histologic process of ossification is periosteal and endochondral in the metatarsals and proximal and middle phalanges. A bone collar forms first around the middle of the cartilaginous diaphysis, followed by invasion of the cartilaginous shaft by a periosteal bud, thus initiating the endochondral ossification that extends in a proximal and distal direction.
The distal phalanx differs in this regard from the other phalanges. The intramembranous and endochondral ossification starts at the tip and extends proximally. Dixey clearly describes the process as a “cap” of intramembranous bone formed at the distal end of the cartilaginous phalanx.16 This cap is then converted into a bony “thimble fitting over the cartilaginous phalanx and enclosing it almost up to its base.”16
Morphologic Development of the Skeletal Elements of the Foot
Embryonic Phase and Early Fetal Phase
Bardeen and, more recently, Olivier provided a detailed morphologic study of the skeletal elements of the foot in the embryonic phase.10, 17 In the 13.5-mm embryo, Olivier describes a
foot with three rays: a principal median ray and two lateral rudimentary rays.17 This tridactylic stage suggests a fanlike growth from the median axis. This primitive foot is digitigrade and in acute plantarflexion, and there is no evidence of angulation of the foot relative to the leg.
foot with three rays: a principal median ray and two lateral rudimentary rays.17 This tridactylic stage suggests a fanlike growth from the median axis. This primitive foot is digitigrade and in acute plantarflexion, and there is no evidence of angulation of the foot relative to the leg.
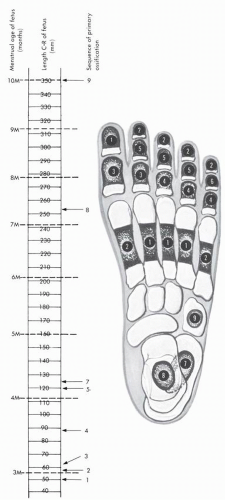 Figure 1.17 Chronologic sequence of ossification of fetal foot. (Correlation of menstrual age and C-R length based on Arey LB. Developmental Anatomy. 7th ed. Philadelphia: WB Saunders; 1965:104.) |
The interosseous slit of the leg is extended onto the ventral aspect by a groove and divides the foot into two parts: preaxial (cranial), comprising the second ray, a rudiment of the first ray, the tarsal elements corresponding to the talus, the navicular, and the cuneiforms; and postaxial (caudal), comprising the third ray, the beginning of the fourth ray, and the tarsal elements corresponding to the cuboid and the calcaneus.17 The fibula is extended by the calcaneus and the three lateral rays.
In embryos measuring 14.2 mm and 17 mm (horizon 18), the foot presents five rays separated fanlike from each other. The foot is sagittal in orientation, with the medial border cranial and the lateral border caudal. The mesenchymal anlages of the distal end of the tibia and fibula in horizon 18 (14 mm) are separated, and the talar element is wedged in between.17 The distal end of the tibia is oblique and concave. Because of the obliquity of the tibial surface, the medial malleolus projects more distally than the end of the fibula (Fig. 1.18). In horizons 19 (17 mm) and 20 (21 mm), the malleoli are at the same level; it is only after horizon 22 (27 mm) that the lateral malleolus extends more distally than the medial. The fibulocalcaneal contact is established early and is clearly present at horizon 20 (21 mm). The tip of the lateral malleolus loses contact with the calcaneus at horizon 22 (27 mm). It is during this period that the distal tibia and fibula come close and establish contact for the formation of a distal tibiofibular joint; this is a relatively late occurrence in the embryonic developmental period.
The talus is delineated at horizon 18 (14.2 mm; see Fig. 1.18).17 The contour is irregular. The element is angled at 90 degrees, with a transverse segment corresponding to the body and future trochlea, and a sagittal segment located inward and inferiorly, corresponding to the neck and head. The superior surface is located between the tibia and the fibula. The element of the talar neck is directed toward the second metatarsal. Only the lateral third of the lower surface establishes contact with the calcaneus (Fig. 1.19). The anterior surface is in continuity with the navicular. The posterior part of the lateral surface has a surface corresponding to the lateral malleolus. The posterior part of the medial surface presents a convex surface (see Fig. 1.18) corresponding to the tibial plafond and the medial malleolus. At this stage “the talus is low, large, and located on the medial flank of the calcaneum over which it overlaps slightly; there is yet no torsion of the head, nor clear declination of the neck.”17
Sudden rapid changes occur in horizon 22 (27 mm). The sustentaculum tali appears, and the talus passes nearly entirely over the calcaneus (see Fig. 1.19). The talus “narrows transversely, elongates but does not elevate yet.”17 The superior talar surface is flat, descending medially and articulating with the tibia. No true trochlea is present yet. At 34 mm, the talus more or less resembles the adult structure (see Fig. 1.19). The foot has pronated. The declination angle of the talar neck-head has increased to 25 degrees. The cephalic torsion has not occurred. The trochlea is narrow; the lateral process is well developed,
supporting the articular surface for the lateral malleolus. The talus is still a relatively flat structure. The navicular has separated from the talar head.
supporting the articular surface for the lateral malleolus. The talus is still a relatively flat structure. The navicular has separated from the talar head.
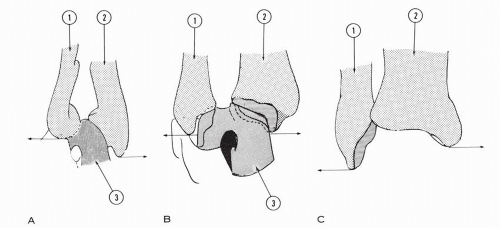 Figure 1.18 (A) Ankle of embryo in horizon 18 (14 mm). The talus is wedged between the tibia and the fibula. The distal end of the tibia is oblique and concave. The distal ends of the fibula and tibia are separated, and the former is proximal to the medial malleolus. (B) Ankle of embryo in horizon 19 (17 mm). The distal tibia and fibula are still separated, and the talus is wedged between the two. The fibular and tibial malleoli are at the same level. The talus is angled at 90 degrees. (C) Ankle of embryo in horizon 22 (27 mm). The lateral malleolus is more distal than the medial malleolus (1, fibula; 2, tibia; 3, talus). (Adapted from Olivier G. Formation du Squelette des Membres. Paris: Vigot Frères; 1962.) |
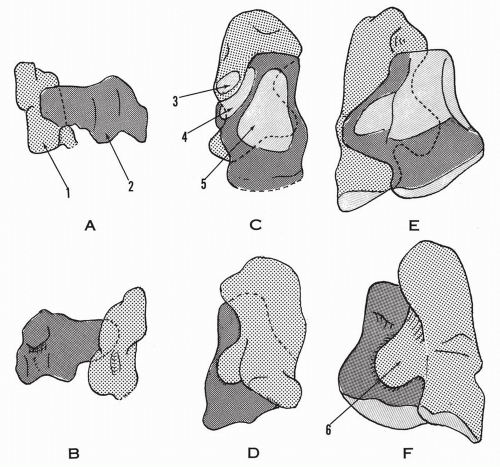 Figure 1.19 Talocalcaneal formation and relationships. Dorsal (A) and (B) plantar views of an embryo of 21 mm. Dorsal (C) and (D) plantar views of an embryo of 27 mm. The talus and the calcaneus overlap. The sustentaculum tali is initiated. The calcaneus presents an articular facet to the distal end of the fibula. The talus is narrower and longer. The lateral and superior talar articular surfaces are initiated but separated. (E) Dorsal and (F) plantar views of a fetus of 34 mm. The sustentaculum tali is well developed. The dorsal, lateral, and medial articular surfaces of the talus have merged. The calcaneal facet for the distal fibula has disappeared (1, calcaneus; 2, talus; 3, calcaneal articular facet for the distal fibula; 4, lateral articular facet of talus; 5, superior trochlear articular facet of talus; 6, sustentaculum tali). (Adapted from Olivier G. Formation du Squelette des Membres. Paris: Vigot Frères; 1962.) |
The calcaneus is initially short, with a narrow superior surface.17 The anteromedial segment of this surface corresponds to the talar overlapping segment; the posterolateral segment gives support to the distal end of the fibula. This small fibular supportive surface, still seen early in horizon 22 (27 mm), fades away, with the lateral malleolus retaining only the talar relationship. The sustentaculum tali, clearly present at horizon 22, extends further medially, and by 34 mm it nears the medial border of the talus. The inferior calcaneal surface presents a large posterolateral tuberosity in horizon 19 (17 mm), and by horizon 20 (21 mm) a posteromedial tuberosity emerges.
McKee and Bagnall18 studied the skeletal relationship of the ankle, hindfoot, and forefoot in six human embryos with a C-R length ranging from 21.7 to 34.0 mm, representing horizon 20 to horizon 23. Three-dimensional reconstruction was used to recreate the skeletal elements of the embryonic foot. The sections were made in three different views of the embryonic foot. When observations were made with the sole of the foot directed downward, as if the foot were in the standard anatomic position, the embryonic calcaneus appeared to be located on the fibular side of the talus with the calcaneus exposed (Fig. 1.20). The tibia extended further plantarward than the fibula, and the medial malleolus was longer than the fibular malleolus. When the relationship of the skeletal elements was reconsidered with the embryonic first metatarsal directed cranially, a completely different relationship was evident. With the forefoot thus inverted, the study of the hindfoot skeletal elements as seen in the coronal sections indicated clearly the calcaneus situated below the talus and the fibula extended further than the tibia, as in the adult foot (Fig. 1.21).
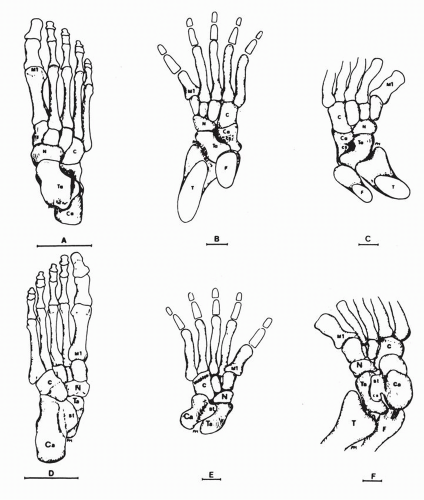 Figure 1.20 Embryonic skeletal elements compared to the adult foot. (A,D) Adult, right foot. (B,E) Embryo XXIIa, right foot. (C,F) Embryo XXIII, left foot. (A-C) Dorsal views. (D-F) Plantar views. (C, cuboid; C1, medial/first cuneiform; C2, intermediate cuneiform/second; C3, lateral/third cuneiform; Ca, calcaneus; cs, calcaneal sulcus; F, fibula; N, navicular; M1, first metatarsal; M2, second metatarsal; M3, third metatarsal; M4, fourth metatarsal; M5, fifth metatarsal; st, sustentaculum tali; T, tibia; Ta, talus). (A,D) Bar = 5 cm. (B,F) Bar = 0.5 mm. (C,F) Bar = 0.5 mm. (After Mckee PR, Bagnall KM. Skeletal relationships in the human embryonic foot based on threedimensional reconstructions. Acta Anat. 1987;129:34.) |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


