1.5 Deep fascia of the lower limbs In the literature, different fasciae such as the fascia lata, iliotibial tract, plantar fascia, crural and gluteal fasciae are described in the lower limbs but only a few words are dedicated to their macroscopic and histologic description. Recent studies highlight the unifying role of connective tissue in the limbs. In particular, these studies have demonstrated the serial continuity of the different fasciae, demonstrating how the gluteal fascia continues with the fascia lata, the crural fascia, and lastly, the plantar fascia. The deep fasciae also blend with the periosteum, tendons, and ligaments (Benjamin 2009). The many functions of the deep fascia of the lower limbs include its role as ectoskeleton for muscle attachments, and the creation of osteofascial compartments for muscles. Its role in venous return, the dissipation of tensional stress concentrated at the site of entheses, and the fact that it serves as a protective sheet for underlying structures has also been recognized. As our understanding of the anatomy and physiology of these structures expands, the important role of the deep fasciae in the interaction among the different muscles of the limbs has become more apparent. The deep fasciae could be considered to be like a bridge, passing over the joints and the septa to connect different muscles, but recent studies (Langevin 2006a) also recognize a primary role in the perception and coordination of movements, due to the unique mechanical properties and dense innervation of these fasciae. Different researches also suggest that the deep fasciae present a basal tension. This basal tension could be due to the stretching of the underlying muscle by muscular or tendineous insertions (Stecco et al. 2009), or by the action of the myofibroblasts within the fascia (Schleip et al. 2006). A few strong intermuscular septa originate from the inner surface of the deep fascia of the lower limbs and extend between the muscle bellies, dividing the thigh into different compartments, and providing an origin to some lower limb muscle fibers (Plate 1.5.1). While the iliotibial tract could be considered the tendon of the tensor fascia lata and the gluteus maximus muscles, it is also a reinforcement of the fascia lata. It has extensive attachments to the lateral intermuscular septum in the thigh and many muscular fibers of the vastus lateralis muscle also originate from this septum. Therefore, during movement of the lower limb, the lateral intermuscular septum is stretched proximally by the gluteus maximus, and distally by the vastus lateralis muscles (Plate 1.5.2). Distally, the iliotibial tract is attached to Gerdy’s tubercle at the upper end of the tibia, but it also has an expansion into the antero-lateral portion of the crural fascia. Fairclough et al. (2007) suggest that iliotibial band syndrome is not due to frictional forces created by moving forwards and backwards over the tibial condyle during flexion and extension of the knee, but to tensional changes within the iliotibial tract itself. Similarly, the sartorius, gracilis, and semitendinosus muscles form the pes anserinus in the medial portion of the knee, but they also extend some expansions into the medial aspect of the crural fascia (Fig. 1.5.1). Besides, the quadriceps muscle has some obliquely directed fascial expansions arising from the vastus medialis and lateralis muscles, that pass anterior to the patella fusing with the fascia lata, and contributing to knee retinacula formation, and the distal tendon of the semimembranosus muscle has two expansions in the popliteal region: one extends into the posterior wall of the knee joint capsule, forming the oblique popliteal ligament, and one extends into the fascia of the popliteus muscle. Distally, the proximal portions of the gastrocnemius muscle are inserted directly onto the fascia, so that these muscular fibers could be considered as tensors of the fascia (Plate 1.5.3), and anteriorly the tibialis anterior muscle and flexor hallucis longus insert onto the overlying fascia and the intermuscular septum. In this way, around the knee, it is quite difficult to separate the deep fascia from the underlying muscles and tendons.
Introduction
Gross anatomy
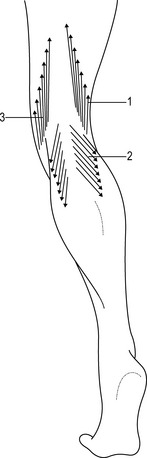
Fibrous expansions and muscular insertions
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Deep fascia of the lower limbs