Custom Triflanged Devices in the Revision Acetabulum
Custom Triflanged Devices in the Revision Acetabulum
Jason M. Jennings
Charlie C. Yang
Douglas A. Dennis
INDICATIONS
With massive bone loss, these custom devices allow acetabular component placement at the correct anatomic level to restore hip biomechanics and stability. The decision to use a custom triflanged acetabular component (CTAC) must be determined preoperatively.
Periacetabular bone loss that precludes the ability to obtain a stable acetabular reconstruction with a traditional hemispheric cup defect-matching technique
TABLE 25-1 Paprosky Classification of Acetabular Defects
Type
Description
1
Columns intact
Hemisphere intact
>70% of prosthesis can be in contact with host bone.
2A
Columns intact
Defect below superior dome
Migration of head center <2 cm
No ischial or tear drop lysis
Kohler line intact
2B
Columns intact
Superior lateral migration creating dome defect
Migration of head center <2 cm
Minimal ischial lysis
Kohler’s line intact
2C
Columns intact
Medial wall defect
Medial migration with minimal superior migration of head center
3A
Columns intact
Severe superior lateral migration creating >50% dome defect
Migration of head center >2 cm
Kohler’s line intact
3B
Posterior column deficient
Severe superior medial migration
Severe ischial lysis
Kohler’s line broken
Possible pelvic discontinuity
TABLE 25-2 AAOS Classification of Acetabular Defects
Type
Description
I
No significant bone loss
II
Columns and rim intact
Contained cavitary loss
III
Columns may be deficient
Uncontained defect involving <50% of acetabulum
IV
Columns deficient
Uncontained defect involving >50% of acetabulum
Pelvic discontinuity may be present.
Physical Examination
Previous incisions
Leg lengths
Motor—particularly the function of the abductor musculature and sciatic nerve distribution
Infection Workup
Traditional—ESR, CRP, and hip aspiration (if indicated)
Supplemental testing—leukocyte esterase (3), synovial CRP (4,5), and IL-6 (6)
Previous Operative Records
Complications or unusual techniques
Type, size, and fixation of current implants
Plain Radiographs
Anteroposterior (AP) view of the pelvis.
Judet and inlet/outlet pelvic views may be helpful in classifying bone loss and determining the presence of pelvic discontinuity.
AP and lateral views of the hip capturing the entire prosthesis.
Full-length orthoroentgenograms may be necessary for preoperative leg length assessment if significant asymmetry is observed.
A preoperative anteroposterior radiograph with traction applied to the operative limb may be helpful to assess laxity of the hip and subsequent determination of where the hip center of the CTAC should be placed.
Computed Tomography
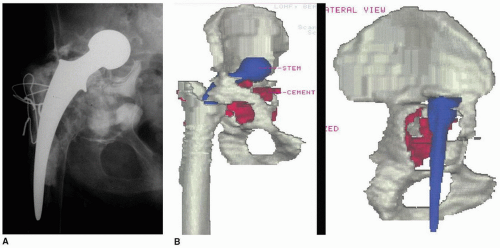
Metal subtraction techniques allow evaluation of osseous defects more precisely (Fig. 25-1A, B).
Specific computed tomography (CT) scan protocols are required for the production of CTAC and should be ordered as such to avoid subjecting the patient to multiple CT scans.
If severe acetabular component protrusion is present, a CT scan with a concomitant angiogram may be required (7). This aids in determining whether intrapelvic vessels or visceral structures are in close proximity to the failed acetabular component. In these cases, a preoperative vascular surgery consultation and consideration of a retroperitoneal exposure to free vital intrapelvic structures from the acetabular component may be warranted.
FIGURE 25-1 A: Anteroposterior radiograph of a failed THA with acetabular component loosening and massive periacetabular bone loss. B: Three-dimensional images created from a thin cut CT scan demonstrating severe acetabulae protrusio and a Paprosky 3B acetabular defect. (From Johnson DR, Dennis DA, Kim RH. Acetabular revision: rings/cages/custom implants. In: Berry DJ, Lieberman JR, eds. Surgery of the Hip. Elsevier; 2013.)
Component Design
The design phase of the CTAC is a critical step. Because the implants are custom made, surgeon input on anticipated further bone removal, hip center, the size and location of the flanged prosthesis, and cup orientation is needed preoperatively. These design decisions have great importance because aside from modular inserts, there are no possible alterations during surgery. The following general steps are utilized to create a custom implant (Fig. 25-2A-G):
Plain radiographs
Thin cut CT (no greater than 3 mm) with metal subtraction
Manufacturer creates three-dimensional (3D) images and a one-to-one computer-aided design (CAD) solid model of the hemipelvis. This model allows for accurate assessment of bone loss and remaining pelvic bone and is utilized to facilitate the design of the CTAC.
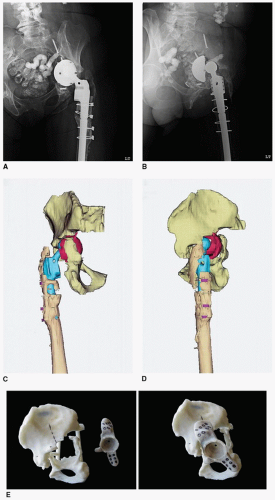
FIGURE 25-2 Preoperative anteroposterior (A) and lateral (B) radiographs demonstrating a failed THA with acetabular component migration and massive periacetabular bone loss. Three-dimensional anteroposterior (C) and lateral (D) images demonstrating severe acetabulae protrusio and a Paprosky 3B acetabular defect. E: Photographs of a one-to-one CAD model of a hemipelvis demonstrating marked periacetabular bone loss along with the acrylic CTAC model designed for the acetabular reconstruction.
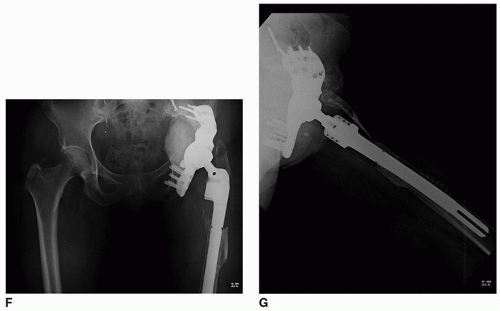
FIGURE 25-2 (Continued) Postoperative anteroposterior (F) and lateral (G) radiographs following reconstruction with a CTAC. (From Johnson DR, Dennis DA, Kim RH. Acetabular revision: rings/cages/custom implants. In: Berry DJ, Lieberman JR, eds. Surgery of the Hip. Elsevier; 2013.)
The surgeon and the design engineer use the 3D model to create a prototype of the CTAC.
The surgeon manipulates the prototype within the 3D hemipelvis and makes recommendations to the design engineer regarding cup orientation, the hip center, and the number and position of the flange fixation screws.
These models can be sterilized and used intraoperatively as a trial component to assess position and fit if needed.
General Design Considerations
The position of the hip center is determined by many patient-specific considerations, including leg length discrepancy, planned retention or revision of the femoral component, length of the contralateral leg, and the size of the current acetabular component. Serving as an approximate anatomic reference, the superior aspect of the obturator foramen is used to determine the vertical head center location. The remaining bone from the anterior and posterior columns determines the head center in the coronal plane. The sagittal plane head center is from the flange geometry and component face diameter. We have found the contralateral hip center, if not distorted by aberrant anatomy or a previous joint arthroplasty, helpful for determining the true anatomic hip center. In cases where the hip center has been displaced superiorly for an extended period of time with a well-fixed femoral prosthesis, it may be impossible to restore the anatomic hip center without neurovascular compromise. In these cases, we will allow some superior positioning of the vertical hip center.
Instability has been reported as a major concern following placement of CTAC (8,9,10,11,12). As such, it is imperative to critically assess the appropriate cup orientation when designing the prosthesis. The abduction angle is set 35 to 45 degrees from the horizontal plane using the plane of the obturator foramen as a reference. The anteversion angle is set at 25 to 30 degrees with the plane of the iliac wing and the obturator foramen as references. Establishing cup face orientation remains a difficult part of the preoperative planning because many of the reference points are often distorted.
Upon finalization of implant design, the surfaces of the titanium alloy stock are milled. The iliac and ischial flanges contain multiple rows of screw holes for cortical or locking screws. Current designs allow for the inclusion of threaded holes to accommodate locking screws into some or all of the holes. We prefer four to six screw holes in the ischial flange because it is proven to be the most common site of fixation loss. We critically assess the geometry of the ischial flange because rough edges or overhang may cause irritation to the sciatic nerve. Two rows of three to four screw holes have proven sufficient for fixation of the iliac flange as this bone typically provides the best purchase. The pubic flange is smaller and does not contain screw holes. Dome screw holes may be placed depending on the adequacy of the iliac bone stock to create interlocking screw fixation with the iliac flange screws. The inner acetabular geometry has a modular locking mechanism that can accept any of the manufacturer specific modular liners typically available for standard acetabular components.
The bone interface of the CTAC, including the flanges, has a porous ingrowth surface for osteointegration. This may be enhanced with the addition of a hydroxyapatite coating. Current CTAC designs allow for easier insertion and provide space behind the implant for additional bone graft at the time of operation. A critical design characteristic is creating a central dome that has intimate contact with the remaining ilium superiorly to reduce shear stresses on the three fixation flange interfaces with bone. In a hip with massive acetabular bone loss or even pelvic discontinuity, this iliac shelf may be the only structurally sound bone available for the construct to rely upon.
Only gold members can continue reading. Log In or Register to continue