CHAPTER 13 Congenital Abnormalities of the Elbow
CAUSES OF CONGENITAL ANOMALIES
Conditions that commonly involve the elbow are constitutional diseases of bone, metabolic abnormalities, and syndromes featuring limb formation and differentiation failures36,38,43,54,82,90 (Table 13-1). Some of the syndromes can be grouped under broad categories such as osteochondrodysplasia,3,29,33,90 dysostoses,18 primary growth disturbances, primary metabolic abnormalities, and congenital myopathies. Most, however, are chromosomal syndromes, from the common dislocation of the radial head69 through fairly well-known syndromes such as trisomy 18, fibrodysplasia ossificans progressiva and the Antley-Bixler syndrome7 to such rarities as the Bruck syndrome (osteogenesis imperfecta with congenital joint contractures) and a congenital mirror movement syndrome. In some cases, the specific gene locus has now been identified; for example, elbow synostosis may also occur in the context of the multiple synostosis syndrome,53 which has been reported in large family groups and is the result of mutations in genes controlling TGF-b synthesis, including noggin, a protein believed to be important in establishing morphogenic gradients.
CLASSIFICATION
A multitissue defect classification can be based on the most obvious and most inhibiting tissue defect known to be present. Some degree of defect in other tissues is also commonly noted. The classification consists of three major categories: (1) bone and joint anomalies, (2) soft tissue anomalies, and (3) anomalies involving all tissues. Bone and joint abnormalities at the elbow may include major absences, but more commonly the skeletal structures are present but malformed. The common bone and joint problems are synostosis (Fig. 13-1), ankylosis (Figs. 13-2 to 13-4), and instability (Fig. 13-5). Soft tissue anomalies include malformations with contractures, control deficiencies, isolated tissue anomalies (Fig. 13-6), and congenital tumors (Fig. 13-7). Complete absence or disorganization of the whole limb, including elbow structures, may occur, as in phocomelia (Fig. 13-8); usually, recognizable though dysplastic structures are present (Fig. 13-9). Similar involvement, although more isolated to the elbow area, occurs in the pterygium syndromes.







With reference to the bone and joint deformities only, it has been useful to many authors to classify them as congenital, developmental, or post-traumatic. As noted earlier, there is much confusion and interplay between these diagnoses, particularly with reference to radial head subluxation or dislocation. In this classification, congenital refers to a primary genetic dysplasia of the skeletoarticular structure of the elbow, resulting in an observed deformity. Other congenital anomalies or a familial history of similar anomalies help confirm this as an etiology. Developmental refers to elbow skeletal structures that are relatively normal at birth but that are then secondarily deformed by abnormal stresses (perhaps from a congenital shortening of the ulna); by paralysis or other limited motion (arthrogryposis); neural, metabolic, endocrine or dyscrasia disturbances (hemophilia, loss of pain recognition, hemochromatosis, and so on); tumor or hamartomatous involvement (fibromatosis, osteochondromata, and so on), and disease (sickle cell anemia, Gorham’s disease, infections). The post-traumatic etiologic grouping is included in this chapter only because of the continuing confusion over early radial head dislocations, which are often post-traumatic, either as a variant of Monteggia fracture dislocation or as a pure dislocation of the soft cartilaginous radial head pulling through the annular ligament (see Chapter 20) and its residua.
Both early and late, dislocation of the radial head is often diagnosed as a congenital subluxation or dislocation, but it often is not. A radial head subluxation or dislocation in an elbow with normal, neural, muscular, and skeletal structures in both elbow and forearm is post-traumatic until proven otherwise; such an elbow with abnormal skeletal forearm structures is probably due to developmental stresses, but additional trauma may play a part. Such an elbow with a synostosis from birth or other skeletal deformity and no evidence of peri-birth trauma is due to congenital causes, but again, trauma may be an additional factor. The confusions highlighted by this classification have been much discussed in the literature.14,20,38,45,51,54,61,70,71,72,79
DIAGNOSIS
BONE AND JOINT ANOMALIES
Synostosis
Synostoses may occur between all or any two of the three bones present at the elbow. The most common synostosis is that between the radius and the ulna proximally in the forearm, near the elbow (Fig. 13-10), but these two bones also may be joined at any point in their paired course in the forearm. Mital55 has classified these synostoses as type I, proximal to the proximal radial physis, and type II, distal to the proximal radial physis. Type II synostoses are more likely to be associated with congenital dislocation of the radial head.45 Cleary and Omer12 suggested a four-level classification scheme, in which Type I is clinically but not radiographically fused with a reduced normal-appearing radial head; Type II is similar but with a clear, bony synostosis; Type III has a hypoplastic posteriorly dislocated radial head; and Type IV has a hypoplastic anteriorly dislocated radial head. Type III appears to be the most common deformity and the one most likely to be associated with significant rotational deformity (almost always pronation). In addition, radiohumeral synostosis, ulnohumeral synostosis, or synostosis among the radius, humerus, and ulna may be present; often, the synostosis is in association with other limb abnormalities, the most common of which is probably ulnar deficiency.30,31,42,57,84 Synostosis may also be associated with fetal alcohol syndrome.84 Incomplete synostosis may occur, but often, this is a radiologic appearance rather than an actual occurrence, because complete radiographic synostosis is usually present by maturity.27,38,50,82 Cleary and Omer’s five cases of type I synostosis are, however, genuine; all of the patients were skeletally mature at the time of final clinical and radiologic review.12

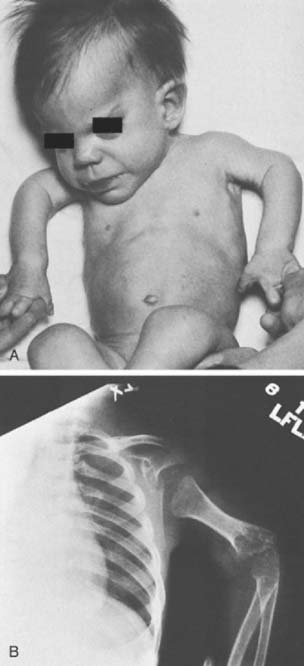
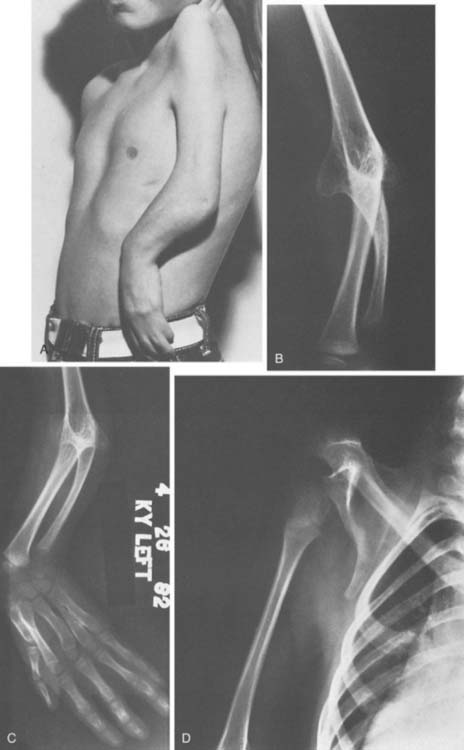
Synostosis between the humerus and either the radius, ulna, or both is less common. Of these, the humeroradial type is most common, followed by humeroradioulnar and humeroulnar types.52 However, anatomy is not the whole story, and McIntyre and Benson52 have proposed an etiologic classification of developmental elbow synostoses, specifically as to whether the synostosis occurs with (class I, or bony type) or without (class II, or joint type) limb hypoplasia. Within each class, the synostosis can be further characterized as occurring in a sporadic or familial pattern and, if familial, with dominant or recessive inheritance. In familial cases, the condition is usually bilateral.12 One of the more dramatic presentations is in the Antley-Bixler syndrome, an autosomal recessive disorder characterized by radiohumeral synostosis, cranial synostosis, midface hypoplasia, and a variety of urogenital and cardiac abnormalities (Fig. 13-10C).7 Distal radioulnar dislocation is a common accompaniment of many of these syndromes.
Ankylosis
Partial ankylosis of the elbow or the proximal radioulnar joint is often overlooked because limited elbow-forearm motion is common in infancy28 and often not remarked in childhood. Causes include failure of complete synostosis, intrinsic abnormalities of the joint or surface formation mechanism, and abnormalities of the surrounding soft tissues, as occurs in pterygium cubitale. The joint must be formed correctly, must have adequate surface material and ligamentous support, and must move soon after its formation, or it will become ankylosed, as occurs, for example, in arthrogryposis, or, far more rarely, in Apert’s syndrome.35,89 There are instances when all or part of the elbow appears to be dislocated but proves to be only malformed and limited in motion (Fig. 13-11). Patients with dysplasia, such as those with Apert’s syndrome, may show a progressive loss of motion over time.89
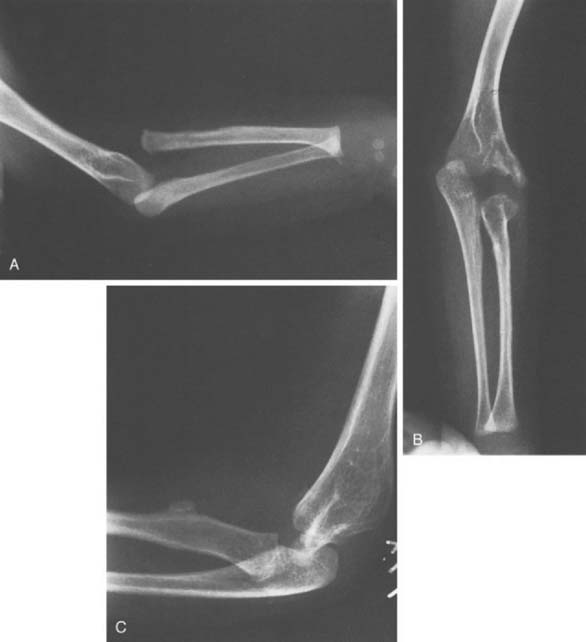
FIGURE 13-11 A, Anteroposterior (AP) x-ray view of an apparent radiohumeral dislocation similar to that shown in Figure 13-2 is seen preoperatively. B, A postoperative AP x-ray view 4 years later shows repositioning of what was determined to be a congenital displaced radiohumeral joint without a dislocation of the radial head. C, A lateral postoperative view of the same elbow. Repositioning was obtained when the radius was shortened by removing a segment of the radial shaft. This segment of excised radius was then used to block the repositioned lateral condyle in its new position. This surgical procedure improved the x-ray position of the elbow but did not change function, which demonstrated both preoperatively and postoperatively mild loss of extension-flexion and moderate loss of supination-pronation.
Instability
The most common problem of instability at the elbow is that of radial head subluxation or dislocation.1,2,11,20,22,25,38,47,48,61,64,67,78,79 When subluxation is an isolated phenomenon, there is considerable doubt about whether it is congenital, developmental, or post-traumatic.14,20,38,45,51 The pulled elbow of infancy is a well-known clinical problem that is associated with trivial trauma and laxity or minor tears of the annular ligament.61,70,72,75 Children have been seen at birth or shortly thereafter with similar problems.14,61,75 Furthermore, such subluxations in the infant, if not treated by closed reduction or other means, may result in deformities similar to those described as indicative of congenital dislocation of the radial head. It has been said that the degree of deformity in the few cases of known infantile dislocation that have been left untreated but followed suggest that the resulting deformity is milder than that seen in definite congenital hypoplasia at the elbow. This may be so but the so-called criteria for classifying a radial head dislocation as congenital (see later) may be seen after any early radial head dislocation regardless of cause (Fig. 13-12). By contrast, when traumatic dislocation is unreduced in the older child, the development of the radial head and the capitellum remains fairly normal, displaying only minimally those radiographic features said to be characteristic of congenital radial head dislocation. These features are (1) a dislocated or subluxed radial head, (2) an underdeveloped radial head, (3) a flat or dome-shaped radial head, (4) a more slender radius than normal, (5) a longer radius than normal, (6) an underdeveloped capitellum humeri, and (7) a lack of anterior angulation of the distal humerus.4,20,56,63,88 Bilaterality, especially symmetric bilateral dislocation, is usually also considered evidence of a congenital etiology, but this is not an absolute requirement.48 However, many if not all the features of congenital dislocation can also be seen with developmental dislocation, due to mild degrees of ulnar or capitellar hypoplasia. In such cases the radial head may slowly dislocate with growth, as the paired forearm bones continue to grow at dissimilar rates.4
There may be only one absolute criterion of congenital elbow dislocation—dislocation with severe hypoplasia of all the osseous elements of the elbow. Absence of the capitellum is probably an example of congenital aplasia, but hypoplasia of the capitellum may occur after dislocation from any cause, as may a deformity of the radial head (see Chapter 20).
When radial head dislocation is familial, bilateral, or seen at birth, or when it occurs with other musculoskeletal anomalies, particularly anomalies in the same upper limb, the evidence is strong that the radial head dislocation is congenital. Cases that are diagnosed later in life may be associated with a discrepancy in length of the paired forearm bones and, therefore, may fall within the “developmental” category. It is well known that inadequate length of the ulna from any cause will result in increased compressive stresses along the radius, gradually leading to a subluxation and perhaps a dislocation of the radial head.38,47,79 Such subluxations, therefore, also may be a secondary phenomenon.48
Approximately half of all patients with isolated congenital radial head dislocation will have a problem bilaterally.2,48,56 Bell and associates4 have classified isolated congenital dislocations of the radial head as type I, subluxation; type II, posterior dislocation with minimal displacement; and type III, posterior dislocation with significant proximal migration of the radius. Type I is the least common dislocation but the one most likely to be associated with pain. Types II and III appear to be roughly equally prevalent. Type III is associated with the most loss of motion, usually supination. Deformity of the radial head without subluxation also has been reported.22 Finally, Wiley and colleagues86 have reported congenital anterior and lateral dislocations.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


