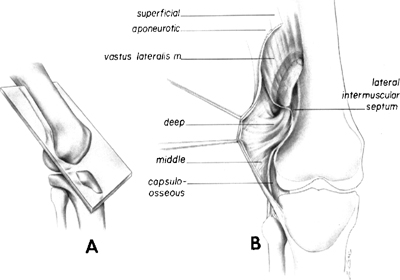
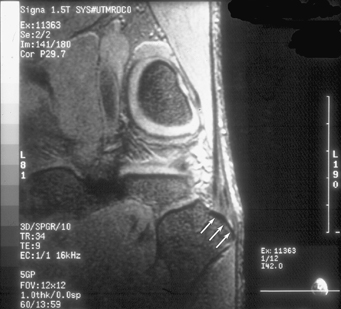
3 It can be argued that one of the biggest sources of confusion in sports medicine is the individual anatomic structures of the posterolateral corner of the knee. Although it has been argued that this is due to multiple factors, including the reported varying incidences of occurrence of the different structures, evolutionary changes over time, and other factors, I believe that most of the problems related to understanding the posterolateral corner of the knee are due to varying dissection techniques and the resulting competing nomenclature for many of these structures. This chapter reviews the standard terminology that has been proposed in peer-reviewed publications, which is based on a consistent anatomic course and attachment pattern, the corresponding relationship to adjacent structures, and descriptions for individual anatomic structures. This review of the individual structures of the posterolateral corner of the knee can be applied in clinical practice to both diagnose injuries clinically and on MRI scans, and to perform repairs or reconstructions of these structures when patients present with pathology. As reviewed in Chapter 2, there have been some evolutionary changes in the anatomic relationships among the fibular head, popliteus tendon, and the biceps femoris muscle that have made the anatomy of the posterolateral corner much more complex than other areas of the knee. At an earlier evolutionary time, the fibular head did articulate with the femur and it gradually migrated distally to its current position, where it articulates with the posterolateral tibial articular surface.1–4 In addition, the popliteus muscle originated on the fibula when the fibula articulated with the femur. As the distal migration of the fibula occurred in higher order animals, the popliteus tendon over time acquired a femoral attachment that appears to be due to development of the remnant of the fibulofemoral meniscus into the popliteus tendon.1–6 In addition, as the proximal fibula migrated distally, it appears to have pulled the lateral capsule distally with it, which, in turn, formed the popliteal hiatus.5 Also, while the popliteus tendon obtained an attachment to the lateral aspect of the femur during the course of evolutionary development, the popliteus complex also maintained its attachment to the fibula (popliteofibular ligament).5 Other factors that have made the anatomy of the posterolateral knee complex and somewhat unique in humans is the change in the insertion of the biceps femoris complex from the lateral capsule and proximal tibia in lower animal species and primates7–10 to attach to the fibula and other posterolateral structures in humans. In all other animal species, the biceps femoris is the main superficial structure over the lateral aspect of the knee. It does not appear that there are any animal species that have a direct attachment of the biceps femoris to the fibula. The other factor that has made the anatomy of the posterolateral knee complex unique in humans is that it appears that only humans have an iliotibial band, which forms the main superficial covering over the anterolateral aspect of the knee.7,11 As reviewed in Chapter 2, the inconsistent terminology in the literature for the posterolateral knee has significantly added to clinicians’ misunderstanding of posterolateral knee anatomy. For example, the “short lateral ligament” has been used to describe the fabellofibular ligament,4,12–15 the popliteofibular ligament,16,17 and the lateral limb of the posterior “arcuate” ligament.18 Kaplan4 summarized the literature and reported that the short lateral ligament and the fabellofibular ligament were homologous structures, with the short lateral ligament present when a bony fabella was absent. Although some authors have found varying incidences of the presence of the fabellofibular ligament,14,19 I believe that this variation was due to the lack of standard nomenclature and to differences in dissection techniques. With our definition of this structure as the distal edge of the capsular arm of the short head of the biceps femoris, and with the understanding that the fabellofibular ligament is tight in extension and becomes quite lax and hard to define with the knee flexed, we have found it to be present in all dissected knees. In addition, the structure was noted to be very difficult to identify in formalin- preserved knees because it is difficult to preserve and dissect it out, as well as because of its thin fascial substance in most knees. Although I have not quantitated it specifically in our peer-reviewed studies, the size and stoutness of the fabellofibular ligament seems to correlate with the presence and size of a bony fabella. In spite of all these differences in nomenclature and evolutionary changes over time, however, the largest source of confusion in the literature about the posterolateral knee was the composition and presence of the “arcuate” ligament.4,12,14–26 Although some authors have reported it to be a separate and distinct structure, I have found it not to be a separate structure, but rather a group of structures. In effect, the previous literature named several different structures located in close proximity as the arcuate ligament and as time evolved and it became recognized that the popliteofibular ligament was a distinct structure, those centers that did not recognize that the popliteofibular ligament had been called the arcuate ligament in the past were now defining it as portions of the capsular arm of the short head of the biceps femoris. Together, these separate individual structures combine to form an arched, or “arcuate,” shape over the posterior aspect of the knee. I would recommend that the term arcuate ligament be dropped due to the confusion created in the past about which structure it refers to. The use of specific anatomic nomenclature for individual structures will help us all perform biomechanical, clinical, and radiographic studies that will lead to better surgical treatment for those patients who have posterolateral knee injuries. In addition, I have noted a lot of difficulty in the identification of the normal attachment sites of the fibular collateral ligament, popliteus tendon, and popliteofibular ligament, which are the main static stabilizers of the posterolateral knee, at the time of acute injury or chronic repairs or reconstructions. The lack of distinct anatomic descriptions and a lack of references to bony landmarks,1,3,5–8,14–20,23,24,26–31 led to our study of the quantitative spatial relationships and attachment sites for these particular structures.32 The iliotibial band, also commonly called the iliotibial tract, is composed of four main structures. An incision over the lateral aspect of the knee exposes the large sheet of tissue that comprises the superficial layer of the iliotibial band. This superficial layer of the iliotibial band covers a large portion of the lateral aspect of the knee. The distal aspects of the iliotibial band converge to primarily attach at Gerdy’s tubercle (Fig. 3-1). A curvilinear anterior expansion of the superficial layer is the iliopatellar band.33,34 The iliopatellar band courses from the main portion of the superficial layer to extend to the lateral border of the patella. The iliopatellar band is important in patellofemoral tracking, and its distal edge, which courses from the distolateral aspect of the patella down to the attachment of the iliotibial band on Gerdy’s tubercle, is the lateral patellotibial ligament. In those patients who receive an overzealous lateral release and end up with symptomatic medial patellar subluxation, a reconstruction of this band can be performed35 to stop this symptomatic iatrogenic medial patellar subluxation. Figure 3-1 The lateral aspect of a left knee demonstrating the superficial layer of the iliotibial band and its iliopatellar band expansion. Figure 3-2 (A) Plane of section. (B) Coronal oblique illustration of the right knee demonstrating the course of the deep and capsulo-osseous layers of the iliotibial band. (From Terry GC, Hughston JC, Norwood LA. The anatomy of the iliopatellar band and iliotibial tract. Am J Sports Med 1986;14:39–45, with permission.) The deep layer of the iliotibial band is medial to the superficial layer and attaches the medial aspect of the superficial layer to the distal aspect of the lateral intermuscular septum of the distal femur.33,34 Deep and posterior to the deep and superficial layers of the iliotibial band, the capsulo-osseous layer of the iliotibial band emerges from deep and more proximal attachments to the lateral head of the gastrocnemius and short head of the biceps femoris muscle to attach just medial and distal to the deep layer of the iliotibial band along the supracondylar area of the lateral aspect of the femur33,34 (Fig. 3-2). From this proximal attachment site on the femur, as well as its attachment sites to these two muscle groups, the capsulo-osseous layer of the iliotibial band continues distally as a fascial sling over the lateral aspect of the joint. It attaches to the tibia just posterior and proximal to Gerdy’s tubercle. This lateral-based sling is what one attempts to reconstruct in extraarticular anterior cruciate ligament reconstructions. The long head of the biceps femoris forms the posterior aspect of the sheet of tissues that cover the lateral aspect of the knee. Overall, the long head of the biceps femoris has six attachments at the knee.36–38 About a centimeter proximal to the lateral aspect of the fibular head and styloid, the long head of the biceps femoris tendon divides into two tendonous components. These are the direct arm and the anterior arm. The direct arm is the distal termination of the majority of the common biceps tendon and inserts on the far posterolateral edge of the fibular head, slightly lateral and distal to the tip of the fibular styloid (Fig. 3-3). The anterior arm of the long biceps has a portion of its substance attaching slightly distolateral to the direct arm attachment on the posterolateral aspect of the fibular head, with the majority of the more lateral substance of the anterior arm continuing distally, where it crosses lateral to the fibular collateral ligament. In this location, a small bursa is located anterolateral to the distal fourth of the fibular collateral ligament. The anterior arm of the long head of the biceps femoris serves as the lateral wall of this bursa. It is a very useful clinical landmark because a small horizontal incision through the anterior arm, 1 cm proximal to the fibular head, allows for direct and consistent access to the attachment site of the fibular collateral ligament on the fibular head (Fig. 3-4). This surgical approach is extremely useful in identifying the injured fibular collateral ligament during a repair or reconstruction. In addition, a suture placed into the substance of the fibular collateral ligament allows for traction to be placed on it and for easier identification of proximal tears, which may be encased in scar tissue or avulsed off the femur.39 Figure 3-3 The lateral aspect of a left knee demonstrating the direct and anterior arms of the long head of the biceps femoris. Hemostat is pointing to the common peroneal nerve (arrow). Figure 3-4 The lateral aspect of a right knee. The anterior arm of the long head of the biceps femoris has been incised to expose the fibular collateral ligament within the fibular collateral ligament/biceps femoris bursa. Figure 3-5 The components of the long head of the biceps femoris of a left knee (anterior arm is held in forceps, anterior aponeurosis continues down leg, lateral aponeurosis is deep to hemostat under [medial] fibular collatural ligament). In addition to these two tendonous components of the long head of the biceps femoris, there are four fascial components: a reflected arm, a lateral aponeurosis, an anterior aponeurosis, and a distal fascial expansion36 (Fig. 3-5). After the anterior arm of the long head of the biceps crosses the fibular collateral ligament, it continues distally and anteriorly and terminates as an anterior aponeurosis over the anterior compartment of the leg. Proximal to the fibular attachment, the anterior edge of the anterior arm provides an attachment for a lateral aponeurotic expansion to the posterior and lateral aspect of the distal aspect of the fibular collateral ligament. In addition, a reflected arm of the long head of the biceps tendon ascends anteriorly, crosses the distal portion of the short head of the biceps femoris, just proximal to the direct arm fibular attachment, and attaches to the posterior edge of the superficial layer of the iliotibial tract. Finally, the posterior aspect of the long head of the biceps femoris tendon has a distal fascial expansion of tissues that attach to the lateral gastrocnemius and sulcus muscles. The main components that are injured in posterolateral knee injuries are usually the two tendonous components, the direct arm, and the anterior arm. These structures may be avulsed off their fibular attachments and retracted proximally in severe posterolateral knee injuries. It is important to attempt to reconstitute their attachment on the lateral aspect of the fibular head to restore normal dynamic function to the biceps femoris complex. In addition, we attempt to repair the lateral aponeurosis back to the fibular collateral ligament in acute injuries so that the normal dynamic function that the biceps femoris has in relation to the fibular collateral ligament can be restored. Although on gross observation it appears that the majority of the short head of the biceps femoris consists of the muscular attachment that courses down to attach to the common biceps tendon, it has several important attachments at the posterolateral corner of the knee. Overall, there are six attachments of the short head of the biceps femoris muscle at the knee.36 The short head of the biceps femoris muscle originates just medial to the linea aspera of the distal femur, and its muscle fibers extend anterior, distal, and lateral to attach to the medial edge of the common biceps tendon. The first attachment component of the short head of the biceps femoris at the knee is this proximal muscular attachment to the anterior and medial aspect of the common biceps tendon (Fig. 3-6). A broad capsular attachment that extends from the short biceps tendon to several structures, including the posterolateral aspect of the lateral joint capsule, a bony or cartilaginous fabella or fabella analogue, and the lateral gastrocnemius complex, is called the capsular arm (Fig. 3-7). The capsular arm is the first main attachment that courses off the short head of the biceps femoris toward the posterolateral structures. This capsular arm is a main component of the biceps femoris complex, which attaches along the posterolateral aspect of the knee. It courses down along the short biceps tendon to attach to the tip of the fibular styloid and forms a large fascial sheath to attach to the posterolateral corner of the knee. In some former studies, the structure has been referred to as part of the “arcuate ligament.”15,18,19,23,24,26 The distal edge of the capsular arm of the short biceps is the fabellofibular ligament.34 Distal to the capsular arm of the short biceps, a third attachment of the short biceps at the knee forms a fascial confluence with the capsulo-osseous layer of the iliotibial band. This fascial confluence forms a Y-shaped anterolateral sling that courses medial to the superficial layer of the iliotibial band and the short head of the biceps femoris, and continues distally to attach on the proximolateral tibia just posterior to Gerdy’s tubercle. This fascial sling has clinical significance in that it was the main component of the structures that were reconstructed in extraarticular anterior cruciate ligament reconstructions. Figure 3-6 The lateral aspect of a right knee demonstrating the course of the main muscle fibers of the short head of the biceps femoris. Figure 3-7 The lateral aspect of a right knee demonstrating the capsular arm of the short head of the biceps femoris (under hemostat) as it courses to the posterolateral capsule and lateral gastrocnemius complex (inferior aspect iliotibial band retracted). Once the short head of the biceps femoris reaches the fibular head and styloid region, there is a direct arm attachment that inserts just lateral to the tip of the fibular styloid (and medial to the direct arm attachment of the long head of the biceps femoris). A distinct tendinous attachment between the short and long heads of the biceps direct arm attachments on the lateral downslope of the fibular styloid can be well visualized on high-resolution magnetic resonance imaging (MRI) scans (Fig. 3-8). In addition to the direct arm tendinous attachment, an anterior arm of the short head of the biceps femoris courses off just proximal to the fibular styloid attachment and passes medial to the fibular collateral ligament and inserts on the tibia 1 cm posterior to Gerdy’s tubercle. This anterior arm attachment on the tibia is at the same location as the meniscotibial portion of the mid-third lateral capsular ligament (lateral capsule).36 This attachment site can be well visualized on coronal high-resolution MRI scans, especially when there is an associated soft tissue avulsion or bony Segond fracture.40 The final attachment of the short head of the biceps femoris at the knee is the lateral aponeurotic expansion. This lateral aponeurotic expansion courses anterior and distal off the distal portion of the short head of the biceps femoris to attach to the posteromedial aspect of the fibular collateral ligament. The main clinically relevant components of the short head of the biceps femoris at the knee are the capsular arm, the anterior arm, and the direct arm. The capsular arm has significance because of its broad fascial attachments over the posterolateral aspect of the knee. These components become lax in flexion and very tight in extension and have not been well studied biomechanically. One of the most common sites of injury that we see is that of components avulsed off the fibular attachment, and we attempt to repair them when they are avulsed in this location. Most commonly, they are avulsed with a tear of the direct arm of the short biceps femoris off the fibular head, with or without a concurrent avulsion of the attachment sites of the direct and anterior arms of the long head of the biceps femoris.41 In these instances, we attempt to repair them back to their anatomic attachment sites on the lateral downslope of the fibular styloid. The most common location that we see with an anterior arm injury is that of an avulsion off the tibia concurrent with a bony or soft tissue Segond injury. In these instances, we attempt a direct repair back to the tibia when we are doing a surgical approach for an acute injury. Because these structures are tight in extension, it would appear that they are functionally important to the prevention of knee hyperextension.
Comprehensive Anatomy of the Structures of the Posterolateral Knee
Iliotibial Band

♦ Long Head of the Biceps Femoris



♦ Short Head of the Biceps Femoris Muscle


Related posts:
 Mechanism and Presenting History of Posterolateral Knee Injuries
Clinically Relevant Biomechanics of Posterolateral Knee Injuries
Complications Associated with Posterolateral Knee Injuries
History of the Nomenclature and Study of the Anatomy of the Posterolateral Knee
Clinical Examination of Posterolateral Knee Injuries
Treatment of Posterolateral Knee Injuries
Mechanism and Presenting History of Posterolateral Knee Injuries
Clinically Relevant Biomechanics of Posterolateral Knee Injuries
Complications Associated with Posterolateral Knee Injuries
History of the Nomenclature and Study of the Anatomy of the Posterolateral Knee
Clinical Examination of Posterolateral Knee Injuries
Treatment of Posterolateral Knee Injuries



