Fig. 1.1.
Weight-bearing AP radiograph of the right knee of a 65-year-old male with medial joint space narrowing, osteophytes, and varus deformity.

Fig. 1.2.
Lateral view radiograph of the right knee of a 65-year-old male.

Fig. 1.3.
Full-length radiograph obtained by stitching images together allows accurate measurement of varus deformity and is an important preoperative view to obtain. The comparison to the patient’s relatively normal contralateral (left) knee highlights the loss of medial cartilage and varus deformity of the right knee.
1.2 Diagnosis/Assessment
Diagnosis of osteoarthritis begins with history and physical exam. Alignment of the knee must be evaluated with physical exam and radiographs. Valgus stress views are useful to confirm full thickness intact lateral cartilage and varus stress views can confirm complete joint space loss medially. A standing PA 45°, or “notch” view, can help distinguish a normal lateral compartment from one with joint pathology (see Fig. 1.4). Severity of varus deformity should be determined preoperatively. It is very important to distinguish a fixed varus deformity from one that is flexible or correctable. Loss of medial joint space can create a pseudolaxity, which may lead to overstripping of the MCL during exposure [1]. A full-length x-ray of the lower extremity in both the anterior/posterior and lateral dimensions is often obtained and may be helpful especially in unusual cases (see Fig. 1.3). It is of great importance that the projection is obtained in neutral rotation.
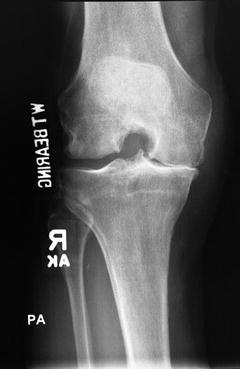
Fig. 1.4.
Standing PA 45° (“notch” view) reveals a normal lateral compartment. This is an important criterion to fulfill to consider a unicompartmental knee arthroplasty. If there was pathology in the lateral compartment, this view would cause the lateral compartment to appear collapsed.
1.3 Management
Management of the varus knee may begin conservatively with oral medication, activity modification, weight loss, and unloader bracing. These efforts may allow the patient to function with a reasonable level of pain control and delay the need for more invasive therapies. As the condition continues to progress, there is a role for glucocorticoid injections, which typically provide a temporary therapeutic benefit in addition to diagnostic value when the pain is relieved by targeted injection. Gel injectables (including synvisc and supartz) are also often administered. When these more conservative modalities fail, patients and providers should consider surgical intervention.
1.4 Outcome
After presurgical evaluation and consent for surgery, the patient in this case presentation underwent medial unicompartmental arthroplasty. The patient began walking within hours after the operation. After 3 weeks of rehabilitation with physical therapy and home exercises, the patient had pain-free range of motion from 2° to 110° with good alignment. At 1 year follow-up visit, the patient was doing well clinically. Radiographs revealed good alignment with no evidence of osteolysis (see Figs. 1.5, 1.6, and 1.7).



Fig. 1.5.
One-year postoperative AP, weight-bearing radiograph of the patient’s right knee revealing good alignment of the unicompartmental knee arthroplasty.
Fig. 1.6.
One-year postoperative PA radiograph of the right knee revealing persistent full thickness joint space of the lateral compartment.
Fig. 1.7.
One-year postoperative lateral radiograph of the right knee obtained in flexion.
1.5 Literature Review
Treatment of varus knee after failure of conservative management has been approached in a variety of ways: proximal tibial osteotomy, medial unicompartmental knee arthroplasty, and total knee arthroplasty. Total knee arthroplasty design construct options include ACL and/or PCL sparing, posterior stabilized, constrained, and rotating hinge.
1.5.1 Proximal Tibial Osteotomy
The proximal tibial osteotomy can be effective in shifting the weight-bearing stresses from the medial to the lateral compartment; however, results are much less immediate than with total knee arthroplasty often taking 6 months for recovery. A meta-analysis demonstrated a good or excellent result at 60 months occurred in 75.3 % of cases, and at 100 months in 60.3 % of cases. Based on these results, the authors suggested that in young patients with specific indications, there is a role for closing wedge tibial osteotomy [2]. However, given the long time frame for recovery and less favorable outcomes (as well as improvements in unicompartmental and total knee arthroplasty), this is a less common surgery, primarily reserved for the young, heavy laborer.
1.5.2 Unicompartmental Knee Arthroplasty
Unicompartmental knee arthroplasty is an important operation to consider in varus knee deformity patients with osteoarthritis affecting only the medial compartment. Patients should fulfill the three Carr Criteria to be considered for unicompartmental knee arthroplasty: a functional ACL, fully correctable deformity, and full thickness of lateral compartment articular cartilage [3]. Several large studies have demonstrated excellent results when patients fulfilling these criteria were selected [4, 5]. Obesity has been reported as another contraindication [6]. Unicompartmental knee arthroplasty has been associated with shorter lengths of stay and lower perioperative complications from this less-invasive procedure, although higher revision rates have been associated with this technique when nationwide databases are analyzed [7].
Related posts:
 Periprosthetic Infection: Management of Late Acute Hematogenous Infection
Complex Primary Total Knee Arthroplasty: Management of Previous Hardware (Posttraumatic OA)
Revision Total Knee Arthroplasty: Management of Deficient Extensor Mechanism
Periprosthetic Infection: Management of Chronically Infected Total Knee Arthroplasty
Complex Primary Total Knee Arthroplasty: Management of Flexion Contracture
Complex Primary Total Knee Arthroplasty: Management of Valgus Knee
Periprosthetic Infection: Management of Late Acute Hematogenous Infection
Complex Primary Total Knee Arthroplasty: Management of Previous Hardware (Posttraumatic OA)
Revision Total Knee Arthroplasty: Management of Deficient Extensor Mechanism
Periprosthetic Infection: Management of Chronically Infected Total Knee Arthroplasty
Complex Primary Total Knee Arthroplasty: Management of Flexion Contracture
Complex Primary Total Knee Arthroplasty: Management of Valgus Knee
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


