Fig. 8.1
Author’s preferred position for isolated or combined PLC/cruciate ligaments reconstruction
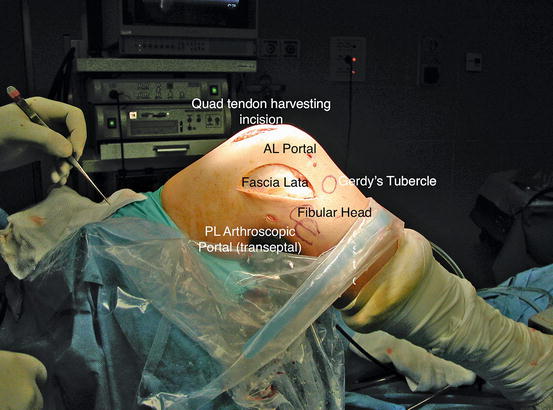
Fig. 8.2
Hockey’s stick incision passing midway between Gerdy’s tubercle and the peroneal head (Note: this patient had already harvested the quadriceps tendon for a PCL reconstruction)
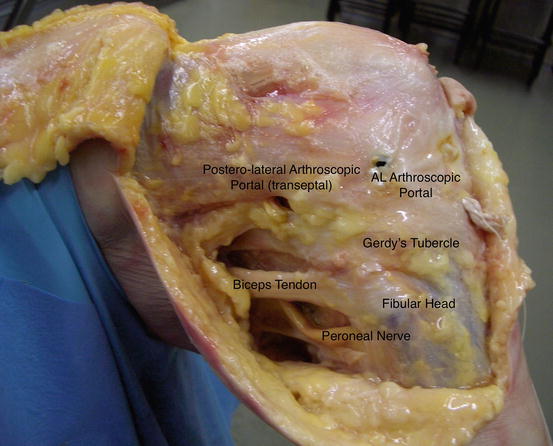
Fig. 8.3
Cadaveric specimen dissection showing the relations existing between the anatomical structures
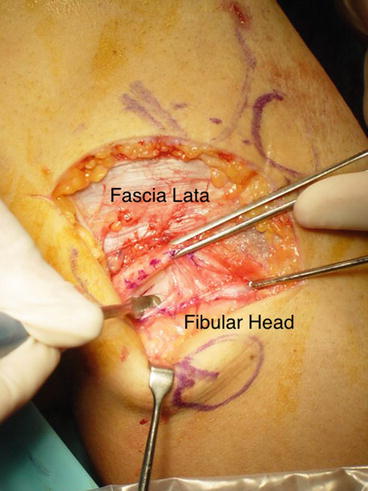
Fig. 8.4
Creation of the transfibular tunnel after dissection and protection of the space behind the fibular head
Then an incision is made in the iliotibial band in line with its fibers directly overlying the lateral femoral epicondyle, which is exposed. The anatomical insertion of the LCL and popliteus tendon is found (Fig. 8.5), and two anatomical tunnels usually 5–6 mm in diameter and approximately 20–25 mm in depth are created (Fig. 8.6). The two tunnels are drilled angled slightly proximal and anterior in order to avoid the intercondylar notch or any tunnels created for concomitant cruciate ligament reconstruction (Figs. 8.7 and 8.8).


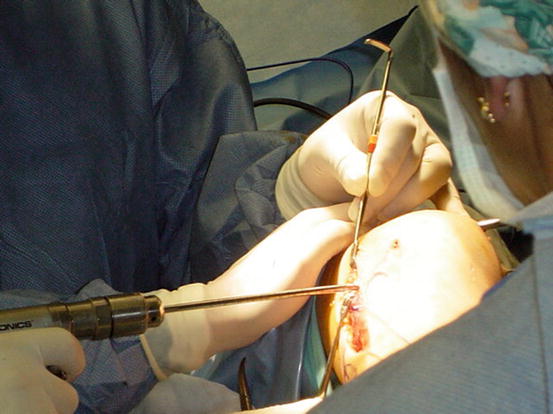
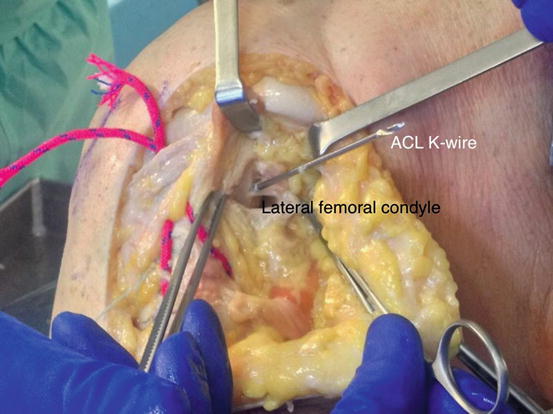
Fig. 8.5
Sometimes it is easy to find a remnant of the ligament that is used, placing the knee in a figure four position, to track the ligament up to its femoral insertion
Fig. 8.6
Placement of the guide wire pro-LCL tunnel. Note the suture (S) wrapping the LCL remnant to better visualize its insertion
Fig. 8.7
A second tunnel is drilled to accommodate the popliteal tendon graft. The direction and inclination of these tunnels should be chosen according to the presence of other concomitant reconstructions
Fig. 8.8
Cadaveric specimen view showing the relationship between the ACL single bundle anatomic tunnel via AM low portal and the PLC reconstruction
A clamp is passed from the epicondyle to the fibular head beneath the IT band. The posterior band is grasped and pulled to the epicondyle, and similarly, the anterior arm is passed taking care to overlap the posterior arm always beneath the IT band, in order to recreate the same anatomical relation existing between the LCL and the popliteus tendon (Fig. 8.9). At this point, the free ends of the grafts are pulled into the femoral sockets by passing sutures that exit the medial aspect of the knee. Graft’s fixation is performed first inserting a bioabsorbable screw within the fibular head, in order to avoid any slippage of the graft when fixing the two bands. Then, two bioabsorbable screws at least 1 mm larger in diameter than the tunnel size drilled are used to fix the two bands of the graft at their entry point into the femur. Alternatively, a button tying the leading sutures on the medial aspect of the knee can be used. The fixation of the two bands is performed with the knee flexed at 30° slightly internal rotation for the popliteus and with a valgus stress applied for the LCL.
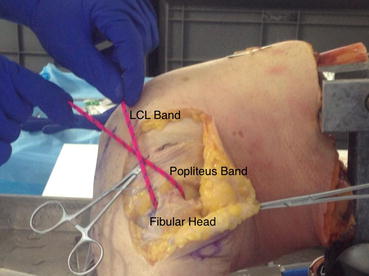
Fig. 8.9




Cadaveric specimen view of the PLC reconstruction. Please note that just for didactical purpose, the graft is placed above the fascia lata rather than below
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
