Chapter 21 Cervicogenic Dorsalgia
After reading this chapter you should be able to answer the following questions:
| Question 1 | What are the two cervical spine structures most commonly linked to production of cervicogenic dorsalgia? |
| Question 2 | What neurologic mechanism has been proposed to account for cervicogenic dorsalgia? |
| Question 3 | What two disorders are most often mistaken for cervicogenic dorsalgia by chiropractors? |
Cervicogenic dorsalgia is pain expressed in the dorsal region and having its genesis in a disordered cervical spine. Although this descriptive phrase locates the anatomic region from which the patient’s symptoms originate, the term cervicogenic dorsalgia is seldom an adequate diagnosis for the doctor of chiropractic. The diagnosis of cervicogenic dorsalgia serves as a rough anatomic locator and it is best accompanied by an indicator of the level of focal segmental dysfunction. If possible, the suggested pathologic nature of the lesion that gives rise to the dorsalgia, for example, subluxation of the C5-6 right posterior facet joint with right cervicogenic dorsalgia, should also be determined. An all-encompassing diagnosis such as this conjures up necessary treatment interventions instantly in the mind of the practicing clinician.
Dorsal pain of cervical origin is frequently observed in clinical practice.1–3 The cervical spine is a freely movable and rather delicate structure sacrificing much in terms of stability for the considerable mobility it enjoys. When one compares the cervical spine possessed of its great mobility with the dorsal spine and its relatively fixed nature, it is easy to comprehend the focal action of static and dynamic stressors on such freely movable segmental structures.
History and Examination
From a historical perspective there is occasionally an obvious clue as to the cervical origin of the patient’s dorsal complaint: “Doctor, when I turn my head to the left I get a stabbing pain in my left shoulder blade.” or “Doctor, I have a heavy pain in my mid back and my neck is stiff and hurts to move in all directions.” This type of historical comment is most often encountered when dorsal pain is of recent origin.
Etiological Mechanism
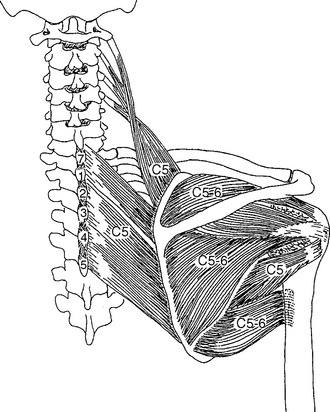
The widespread distribution of signs and symptoms resulting from spinal muscle and joint dysfunction, including subluxation syndromes, may be explained by this mechanism. For example, pain or paresthesia perceived in the anterior or posterior chest, the shoulder, and/or down the arm may be due to irritation of the C7 zygapophyseal joint. Terrettt3 notes that “the posterior thorax is interesting in that interposed between the thoracic dermatome (the skin) and the thoracic sclerotome and myotome (the ribs and intercostal muscles) lies part of the C5-C7 sclerotome (Figure 21-1) and C3-C6 myotome (Figure 21-2).”
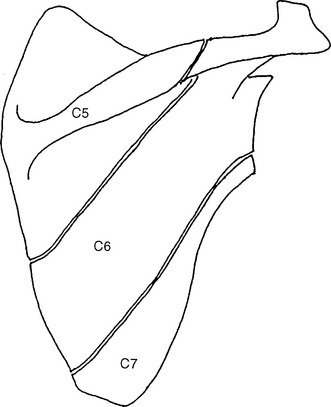
Figure 21-1 C5, C6, C7 sclerotomes of the scapula.
(From Terrett AGJ, Terrett RG. Chiro J Aust 2002;32:42-51.)
Pain Referral Patterns
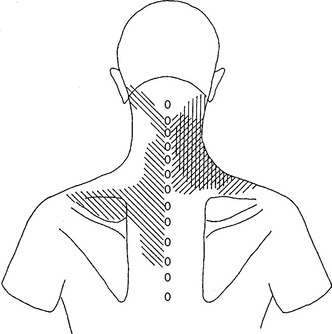
Pain referral patterns have been mapped in studies involving irritation of posterior rami innervated tissues at the C4-5, C5-6, and C6-7 levels. Figures 21-3, 21-4, and 21-5 illustrate these referral patterns. On the left of each diagram are the referral pain patterns from irritation of paravertebral muscles,4,5 and on the right side are the referral pain patterns from irritation of the zygapophyseal joints.6–8






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


