18 Cervical disk degeneration is a normal part of aging and is found in ~ 85% of individuals by the seventh decade of life. Although most people do not have major symptoms resulting from the degenerative process, a subset develop neck or arm pain and may require medical intervention. The term radiculopathy denotes the constellation of symptoms caused by compression and/or inflammation of a nerve root, including radiating arm pain, sensory changes and/or motor loss. Nonsurgical treatment is the mainstay of treatment for most patients with neck pain and is the initial treatment offered to patients with symptoms of radiculopathy. Those who fail to respond and have continued severe radicular symptoms are candidates for surgical intervention. The usual underlying pathology involves compression of the neural elements by a combination of herniated disk material and/or osteophytes secondary to spondylosis. The pathophysiology of cervical disk degeneration involves dehydration of the nucleus pulposus and weakening and fissuring of the annulus fibrosus. This combination may allow herniation of nuclear material into the spinal canal or neural foramen. Additionally, the specialized uncovertebral joints of Luschka may form bony osteophytes that compress the cervical nerve roots as they enter the neural foramen. Patients with cervical radiculopathy will classically present with complaints of pain radiating from the cervical region and down the arm along a particular dermatomal distribution. There are often associated symptoms of sensory changes (numbness or tingling) or weakness. The pain is often described as sharp, shooting, lancinating, or numbing. There is frequently associated pain along the medial border of the scapula. A complete spinal and neurologic physical examination should be performed. Affected patients will commonly exhibit decreased range of motion and avoid neck positions (extension and/or rotation) that aggravate the pain. It is common to note minor changes in strength and sensation that are related to the affected nerve root. The reflex arc of the affected nerve root is generally depressed. A Spurling test (cervical extension, rotation, and lateral bending toward the affected side) or axial compression will usually reproduce or worsen the radicular pain. Axial traction generally lessens radicular pain. A differential diagnosis should be considered, including shoulder pathology, brachial plexopathy, peripheral nerve entrapment, or coronary artery disease. Plain radiographs will often demonstrate disk space narrowing and osteophyte formation. Magnetic resonance imaging (MRI) is the most useful study in patients with radiculopathy and can be used to show disk herniation, foraminal narrowing, and neural element compression. Computed tomography (CT) with myelography can be utilized in patients unable to undergo MRI. In the absence of major neurologic loss, conservative measures should be pursued initially. Conservative care includes activity modification, anti-inflammatory drugs, gentle active exercises, cervical traction, and spinal injections. Acute radiculopathies often respond to conservative measures, although the potential for recurrent symptoms exists. Indications for surgical management for cervical radiculopathy generally include severe pain despite 6 to 12 weeks of conservative therapy or progressive/severe neurologic deficits. Surgical intervention can be pursued with one of four available treatment approaches: anterior cervical discectomy and fusion (ACDF), anterior foraminotomy, anterior cervical discectomy and artificial disk replacement, or posterior cervical foraminotomy. Each approach has certain advantages and disadvantages. At the current time, the ACDF approach is the most common surgical procedure done for cervical radiculopathy worldwide. Up to two-thirds of those with radiculopathy obtain improvement with conservative measures. Patients failing to respond have a high success rate for surgery, with rates of arm pain relief in many studies ranging from 85% to 95%. Complications of treatment include recurrent symptoms (with nonoperative care or foraminotomies), swallowing problems, vocal cord paralysis, and adjacent segment degeneration. Boden SDWS. Nonoperative management of cervical disc disease. In: Camins MB, O’Leary PF, eds. Disorders of the Cervical Spine. Baltimore, MD: Williams & Wilkins; 1992:157–164 This is a good review of the history, clinical examination, and management of cervical disk disease. Davidson RI, Dunn EJ, Metzmaker JN. The shoulder abduction test in the diagnosis of radicular pain in cervical extradural compressive monoradiculopathies. Spine (Phila Pa 1976) 1981;6(5):441–446 PubMed This study describes patients with cervical radiculopathies who experienced relief of their symptoms with abduction of the shoulder. Heller JG. The syndromes of degenerative cervical disease. Orthop Clin North Am 1992;23(3): 381–394 PubMed This study describes the patho-anatomic changes in the cervical spine that lead to clinical radicular and myelopathic symptoms. Jenis LG, An HS. Neck pain secondary to radiculopathy of the fourth cervical root: an analysis of 12 surgically treated patients. J Spinal Disord 2000;13(4):345–349 PubMed This article describes the results of surgical intervention in a series of patients with radicular neck pain from involvement of the C4 nerve root. Swezey RL, Swezey AM, Warner K. Efficacy of home cervical traction therapy. Am J Phys Med Rehabil 1999;78(1):30–32 PubMed This article describes the treatment and outcome of cervical radiculopathy with traction.
Cervical Radiculopathy
![]() Workup
Workup
History
Physical Examination
Spinal Imaging
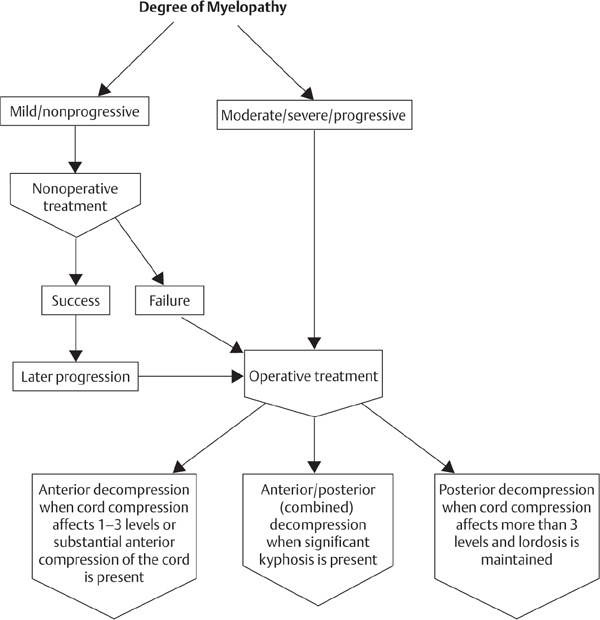
![]() Treatment
Treatment
![]() Outcome
Outcome
![]() Complications
Complications
Suggested Readings
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


