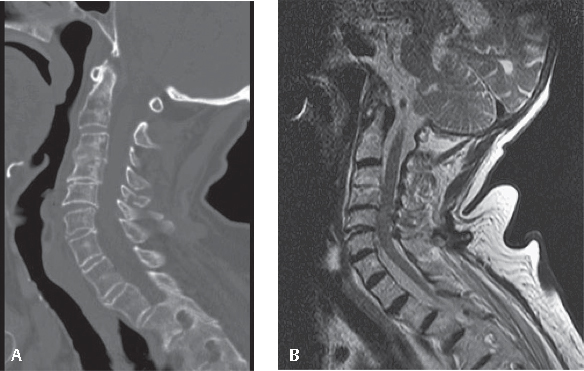
7 Cervical distraction-extension injuries (CDEIs) are responsible for 5–22% of all structurally significant traumas to the subaxial cervical spine. Surprisingly, there are relatively few published studies regarding the CDEI pattern. The majority of CDEIs occur in elderly patients with spondylosis or in patients with ankylosing spondylitis or diffuse idiopathic skeletal hyperostosis (DISH). The common factor for all these diseases is that the flexibility of the cervical spine is dramatically decreased. A CDEI is generally caused by hyperextension of the stiff cervical spine, especially following motor vehicle accidents or falls. The hyperextension forces disrupt the anterior longitudinal ligament (ALL) and disk and may, in severe cases, result in disruption of posterior ligamentous structures. In severe cases, where the posterior longitudinal ligament and facet joint capsules are involved, posterior translation of the superior vertebral body with respect to the subjacent vertebrae will be noted on the lateral radiograph. Such translation markedly compromises the stability of the cervical spine. Neurologic and vascular complications may occur in cases with significant displacement or angulation. Mild cases of CDEI require a high index of suspicion, as the spine may show minimal or no displacement because of a spontaneous postural reduction of the injury. Elderly patients with a history of a significant traumatic mechanism and spondylosis should be examined for this type of trauma. In such cases, magnetic resonance imaging (MRI) scanning can be a valuable tool; high T2-weighted signal within the disk space is consistent with the traumatic disruption. CDEI as classified by Allen and Ferguson has been divided into two stages. In stage 1 CDEI, the disruption involves the ALL and disk (with or without an adjacent vertebral fracture) and one may observe widening of the anterior disk space (Fig. 7.1A,B). In a stage 2 CDEI, the disruption additionally involves the posterior ligamentous structures and leads to retrolisthesis of the superior vertebral body (Fig. 7.2A,B). These more severe injuries are severely unstable, with a higher risk of neurological injury. Samartzis et al.1 studied a cadaver model with serial disruption of the ligamentous structures and expanded the CDEI classification into four categories (DES-1, DES-2A, DES-2B, and DES-3), based on the degree of posterior translation and angulation noted on the lateral radiograph (Table 7.1). Fig. 7.1 85-year-old woman with cervical spine trauma following a ground-level fall. (A) Sagittal CT reconstruction. Notice the preexisting spondylosis resulting in a stiff cervical spine. A subtle widening of the anterior disk space is seen at the C5–C6 level. (B) MRI showing increased T2-weighted signal within the C5–C6 disk space (arrow), which is indicative of the disruption. Using the Allen–Ferguson classification, this would be a Type 1 injury. Table 7.1 Classification of Subaxial CDEI Stages Based on Soft-tissue Injury
Cervical Distraction-Extension Injuries
![]() Classification
Classification
Staging | Soft-Tissue Injuries | Radiographic View |
CDEI-1 | ALL | Angulation |
CDEI-2A | ALL and disk | Angulation and posterior translation |
CDEI-2B | ALL, disk, and PLL | Angulation and posterior translation with instability |
CDEI-3 | ALL, disk, PLL, and facet capsule ± remaining PLL | Angulation and posterior translation with gross instability |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


