12
Carpal Tunnel Syndrome
Kevin D. Plancher
History and Clinical Presentation
A 46-year-old right hand dominant woman presents with symptoms of numbness 5 cm proximal to the right wrist crease as well as loss of sensation in her palm over the thumb area. She noticed her hands go to sleep while driving her car. Her symptoms have been present for 4 to 6 weeks, and have been progressively getting worse. The patient denies cramping in her hand and has no palmar hypersensitivity. She needs to shake her hands out at night and experiences numbness or tingling to the fingertips. The patient spends ∼6 hours a day working on a computer.
Physical Examination
A positive Tinel’s sign is present directly over the palmar cutaneous branch of the median nerve, which the patient says simulates her numbness and tingling to the thenar eminence. In addition to this, she has an area of numbness of 3 × 2 cm directly over the area of innervation at the palmar cutaneous branch of the median nerve in her palm. Her Phalen’s test is positive and her Tinel’s test to the wrist is negative. Her median nerve compression test is positive and her Weber static two-point discrimination is greater than 1 cm to all her median innervated digits. The patient’s grip strength is 110 on the left and 110 on the right on the Jamar dynometer. Pinch is 18 pounds on the left and 18 pounds on the right. All measurements are an average of three trials.
PEARLS
- Avoid the limited open technique in patients with distorted anatomy, fracture of the distal radius, or fracture dislocation of carpus.
- Avoid this technique in patients with marked thenar wasting, or complete or near loss of sensory perception.
- Always extend the excision proximally to allow adequate visualization if limited technique does not provide direct visualization.
Diagnostic Studies
Radiographs are negative for bony or soft tissue abnormalities. Electromyograms (EMGs) show nerve conduction velocities significantly slowing at the median nerve distribution more on the sensory fibers, even to the index with proximal conduction and ulnar conduction normal.
PITFALLS
- Do not use this technique in recurrent carpal tunnel syndrome for a repeat procedure when an open procedure was done previously.
- Never exert force in passing instruments across the ligament without good visualization to avoid cutting the median nerve.
Differential Diagnosis
Carpal tunnel syndrome
Neuroma
Arthritis
Thyroid disease
Diabetes mellitus
Tenosynovitis
Gout
Diagnosis
Moderate Carpal Tunnel Syndrome with Compression of the Palmar Cutaneous Branch of the Median Nerve
Carpal tunnel syndrome is one of the most common conditions of the hand. Swelling of the median nerve or compression of the median nerve by surrounding structures causes sensory and motor disturbances (Fig. 12–1). Chronic repetitive stress on the carpal tunnel and the median nerve within it is the most common cause of idiopathic carpal tunnel syndrome. Occupations that require stress on the wrist, such as typing and carpentry often lead to a high incidence of carpal tunnel syndrome. Sporting activities that involve repetitive or continuous flexion and extension of the wrist, such as cycling, throwing sports, racquet sports, archery, and gymnastics, also predispose individuals to carpal tunnel syndrome.
Carpal tunnel syndrome can be diagnosed by obtaining a careful patient history. Common complaints include nocturnal paresthesia, a heavy feeling, or hands going to sleep. Pain may radiate up the arm to the shoulder and neck. Patients also complain of weakness that hinders their ability to grasp objects. Numbness when gripping objects may prevent the patient from being able to lift objects.
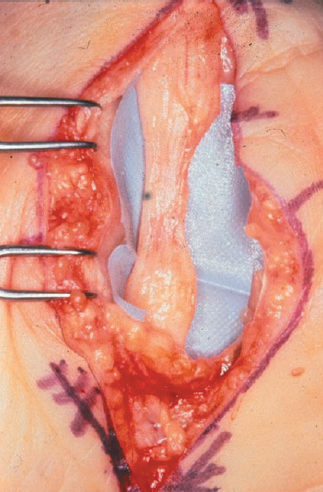
Nonoperative treatments include activity modification, splinting (Fig. 12–2), magnetic support wraps, and injections (Fig. 12–3). In younger patients with early stages of carpal tunnel syndrome, these modalities may relieve symptoms. Following failed conservative treatment, patients may require surgical intervention to regain lost function. Open carpal tunnel release has been shown to relieve symptoms of median nerve compression for many years (Fig. 12–4). Endoscopic carpal tunnel release was shown to reduce tissue trauma and speed postoperative recovery. However, the endoscopic technique requires extensive equipment and has a steep learning curve. In our patients, we perform a limited open incision carpal tunnel release. This technique combines the advantages of the open procedure with the advantage of reduced tissue trauma and postoperative morbidity of endoscopic release.