87
Benign Vascular and Malignant Vascular Tumors
Earl W. Brien and Stuart H. Kuschner
History and Clinical Presentation
Case A. A 35-year-old right hand dominant woman complains of a painful mass about the tip of the index finger of 6 months’ duration. She states that the pain is aggravated by cold and often radiates proximally after tactile stimulation. She denies any history of trauma, puncture wounds, or fever.
Case B. A 55-year-old right hand dominant woman with a history of swelling about the left upper extremity after radical mastectomy and lymph node dissection 10 years prior complains of a painless, enlarging mass in the left hand of 4 months’ duration. She denies any history of trauma, puncture wounds, or fever.
Physical Examination
Case A. The patient has 1.5-cm, firm, nonmobile mass about the tuft of the index finger. The lesion revealed a blue-red hue subungual. She has lancinating pain proximally upon pinprick about the digit. She has no proximal adenopathy and the remainder of her examination is within normal limits.
Case B. The patient has 2.5-cm dorsoradial wrist mass superimposed on a nonpitting, brawny edema. It is firm, superficial, nontender, and nonmobile, without any warmth or erythema. The lesion did not transilluminate and there was a purple hue about the skin. She has full range of motion of the wrist and hand and is neurovascularly intact to all digits. She has no proximal adenopathy and the remainder of her examination is within normal limits.
Diagnostic Studies
Case A. Anteroposterior, lateral, and oblique radiographs of the hand show a soft tissue mass about the tuft with a well circumscribed scalloping about the distal phalanx (Fig. 87–1).

Figure 87–1. Well-circumscribed lesion, distal phalanx.
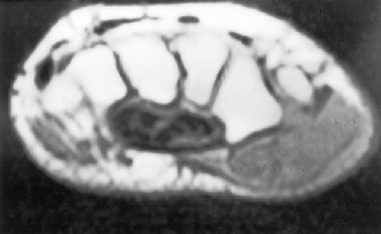
Figure 87–2. Magnetic resonance imaging through the base of the hand of a dorsoradial mass.
Case B. Anteroposterior, lateral, and oblique radiographs of the hand show a soft tissue mass dorsally without calcification. Magnetic resonance imaging (MRI) (Fig. 87–2) reveals a 2.5-cm mass, intermediate signal on T1- and bright signal on T2-weighted imaging. Laboratory studies were unremarkable.
Differential Diagnoses
Case A
Glomus tumor
Melanoma
Inclusion cyst/foreign body granuloma
Infection
Metastatic squamous carcinoma of the lung
Case B
Ganglion cyst
Giant cell tumor of the tendon sheath
Soft tissue sarcoma
Other benign tumors
Atypical infection/synovitis
Inclusion cyst/foreign body granuloma
Pathologic Examination
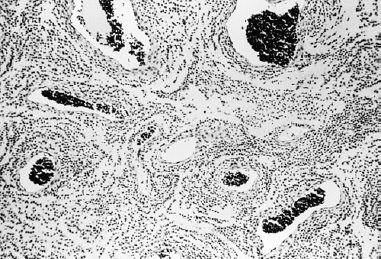
Case A. Histopathologic examination revealed small round blue cells forming vascular structures in a myxoid stroma (Fig. 87–3). On high power (Fig. 87–4), central clearing or punched out nuclei are seen surrounded by a faintly staining cytoplasm best seen with periodic acid-Schiff (PAS) stain or toluidine blue stain. Ultrastructural findings reveal myofilaments closely related to smooth muscle.
Case B. Histopathologic examination (Fig. 87–5) revealed communicating vascular channels dissecting between the dermal collagen and fat cells. Cells lining the lumina reveal hyperchromatic nuclei and mild to moderate atypia with occasional shedding of cells into the lumen. Immunohistochemical stains revealed vimentin and factor VIII antigen positivity.