1 Basic Principles of
Auricular Acupuncture
H.-U. Hecker, A. Steveling,
E.T. Peuker, B. Strittmatter, T.J. Filler

Introduction
Auricular acupuncture represents a special form of acupuncture and is often used as a complement to body acupuncture.
It is based on a self-contained model of thought. A core idea is the concept of somatopy. This expression is composed of the Greek words soma (= body) and topos (= location) and means the differentiated mapping of the body in one area (here the auricula). Often the term microsystem is used synonymously, although strictly speaking this includes the whole diagnostic and therapeutic concept. Somatopies are familiar from different parts of the central nervous system, for example locomotor somatopy in the Gyrus precentralis or sensory somatopy in the Gyrus postcentralis. By means of somatopy, corresponding constructs are also found for other senses, such as tonotopy for hearing and retinotopy for sight.
As a rule, somatopic assignments are not relative to the size of the mapped region but in accordance with the expression of the respective qualities. Thus, in some cases in the central projection areas there are grotesquely disproportionate representations of the body that are often referred to as homunculus. It is a similar story for the familiar microsystems. The representation of the body on the ear vaguely calls to mind an inverted fetus, the proportions and location of which vary considerably, however, depending on the school of auricular acupuncture (see below).
Unlike body acupuncture, the points on the auricula are only irritated and thus identifiable if there is a disturbance in the respective region of the body of which they are a representative projection. This basic principle also applies to the other microsystem zones.
Therapeutic procedures involving the auricula have been mentioned since antiquity. Thus, Hippocrates is said to have tried to cure impotence by means of bloodletting from the outer ear; Egyptian sailors are said to have tried to improve their sight for navigation by pricking their ear lobes (among other things, the Eye Point in the modern auriculotherapy model is also found in the ear lobe).
Time and time again, cauterization of the auricula was undertaken as a therapy for sciatic pain. We know of corresponding applications by, for example, Persian healers. But in Western Europe there are also references to such therapeutic approaches. Thus, as far back as 1637, Zactus Lusitanus described cauterization of the ear as a therapy for sciatic pain in Portugal; in 1810 Ignaz Colla described cauterization of the rear side of the auricula for the same reason. In 1717, Valsalva treated toothache via the auricula. In the second part (Ling Shu) of the Huang Di Nei Jing, there are observations regarding treatment in the area around the auricula. However, beyond this there are no references to a concept of auricular acupuncture by the standard authors of Chinese medicine.
As early as the 18th century, numerous publications reported the benefits of cauterization of the auricula as a therapy for sciatica. However, it was not until 1950 that the French neurologist Paul Nogier attempted to write a comprehensive description of the therapy of the auricula. He discovered cauterization marks on the anthelix in numerous patients who had been treated by a healer (Mme. Barrin) for sciatic pain. The patients reported astonishing success with this therapy, leading Nogier to further investigate the phenomenon. He also began his own trials with cauterization but then turned to “less barbaric” methods such as pricking with needles or pins, with which he achieved equally good results. He came to the conclusion that disturbances of the body (over and above sciatic pain) could be demonstrated on a regular basis by means of sensitive or painful points on the auricula. He interpreted the representation of the body on the auricula as the image of an inverted fetus–he was thus able to assign the point on the antihelix usually used for sciatic pain therapy the representation zone L4.
In February 1956, at the invitation of the famous acupuncturist Niboyet, Nogier presented his findings at the first congress of the Société méditerranéenne d’Acupuncture in Marseilles, France. At the instance of Gerhard Bachmann (then Chairman of the Deutsche Gesellschaft für Akupunktur [German Society for Acupuncture]), these findings were published in the Deutsche Zeitschrift für Akupunktur (German Acupuncture Journal) in 1957. The findings were not known about in China until the beginning of 1959. Here, although in the past the auricula had been regarded as an important topographical region at which some meridians of body acupuncture meet, independent auricular acupuncture had not previously existed. It was not until the end of 1959 that the expression auricular acupuncture (er zhen) first appeared in Chinese acupuncture literature. Subsequently, “Chinese auricular acupuncture” developed with its own nomenclature and mapping of the ear points which in Europe was employed and interpreted by König and Wancura using a numeric system. Less and less mention is made of the basis of this Chinese auricular acupuncture (the findings of Paul Nogier) in more recent Chinese tutorials.
Nor are there any references in the classic works of Chinese medicine to the microsystems prevalent to a greater or lesser degree in diagnosis and therapy. As a rule, all theories about microsystems are a few years to decades old and have in some cases been implemented retrospectively in one or more of the systems of Chinese medicine.
Taking as a basis the publication of the findings of Paul Nogier in the Deutsche Zeitschrift für Akupunktur, translations or abstracts were also published in Japan, what was then Ceylon (today’s Sri Lanka), and the former USSR.
Today there are several schools of auricular acupuncture; besides the establishment of schools based on Nogier and Bahr on the one hand, and the Chinese school on the other, there has been increasing research activity by Russian scientists based on R.A. Durinjan and F.G. Portnov.
The slight variations in point localizations and approaches in diagnosis and therapy which exist in part between the different schools must not be regarded as rivaling each other, but rather interpreted on the basis of the respective model and the practical approach. Thus, in part, Chinese points represent functional relationships, the Nogier points rather the anatomical correlative. Lastly, a careful investigative technique is crucial for auricular acupuncture in order to identify the individually active points and thus be able to employ them for therapy.
In this book, both the common laws and the differences in the localization of points are described and interpreted, providing the therapist with alternatives which upon closer examination prove to be an enrichment of the range of therapies.
Basic Principles
Anatomy of the Outer Ear (Auricula)
The outer ear together with the auditory canal forms the auricula. Its shape corresponds to the underlying elastic cartilage close to the skin. Only the ear lobe contains no cartilage. Over the dorsomedial area, the skin of the auricula is thin and can be moved relatively easily with regard to the perichondrium. Anterolaterally, the skin is firm and relatively difficult to move.
Both external muscles and own muscles are attached to the auricula. The external muscles permit some people to obtain residual movement of the ear and form part of the mimetic musculature. The ear’s own muscles correspond to the remains of a sphincter system with which the auditory canal can be closed in animals which live in water or underground.
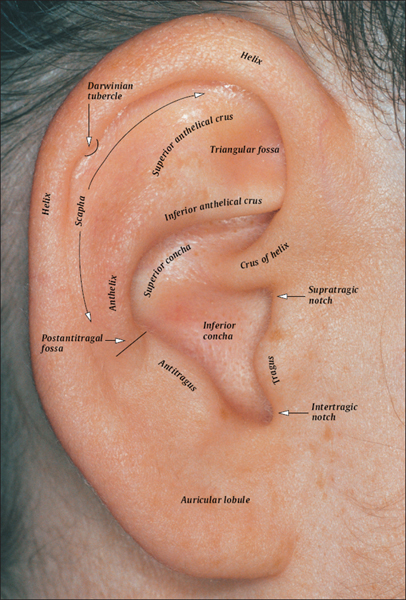
Although the individual internal shape of the ear may vary greatly (and also when the two sides are compared), there are some anatomical landmarks which are relatively constant and can thus serve as reference points for locating the acupuncture points of the ear.
The outer shape of the auricula is formed by the helical rim (helix). The helix originates on the floor of the concha and ascends as the root of helix (crus of helix). It is followed by the body of the helix which descends as the tail of the helix toward the ear lobe. The helix then turns into the ear lobe (auricular lobule). In the upper, rear part of the helix, we usually find a protrusion or widening of the helical rim, the helical tubercle (Darwinian tubercle), which corresponds to the tip of some mammals’ ears. The anthelix runs parallel to the helix. It originates in the upper part of the auricula with two legs, the inferior anthelical crus and the superior anthelical crus. Between the two anthelical crura lies the triangular fossa. The anthelix turns into the antitragus in the lower part of the ear. The border between them is formed by the postantitragal fossa.
Between the helix and the superior anthelical crus plus anthelix lies the scapha.
The tragus is bordered by the intertragic notch to the antitragus and the supratragic notch to the crus of helix. At the bottom of the auricula lies the cavity of concha. The concha is divided by the ascending crus of helix into two parts, the superior concha (cymba) and the inferior concha. The outer auditory canal lies in the inferior concha and is covered from view by the tragus.
The anatomical landmarks of the outside of the auricula partly find their correlate on the rear side. Thus, on the dorsal side of the auricula the helical rim and the eminence of scapha of the sulcus anthelicis can be directly delimited medially. Dorsally both parts of the cavity of concha become the superior and inferior eminence of concha, which are often separated from each other by a sulcus posterior centralis. The equivalents of the crura anthelices (as sulci) and the triangular fossa (as eminentia) on the dorsal side can less frequently be delimited so clearly.
The usually biconcave reverse side of the ear lobe is called the fovea retrobularis.
Zones of Auricular Innervation and Embryological Assignment According to Nogier
Although Nogier did not carry out any anatomical or embryological investigations of his own, several assignments can be found in his records, usually with reference to the research done by Valsalva. According to this, the auricula is innervated by three nerves:
 The auricular branch of the vagus nerve
The auricular branch of the vagus nerve
 The auriculotemporal nerve of the trigeminal nerve
The auriculotemporal nerve of the trigeminal nerve
 The great auricular nerve of the cervical plexus.
The great auricular nerve of the cervical plexus.
The auricular branch of the vagus nerve innervates the concha. According to this concept, the “entodermal” organs are projected here.
The great auricular nerve of the cervical plexus supplies the lobule, the outer helical rim up to approximately the Darwinian tubercle, and the back of the ear. These areas correspond to organs in the ectodermal germ layer. The remaining, and by far the largest, part of the ear is innervated by the auriculotemporal nerve of the trigeminal nerve. The mesodermal organs are projected here.
According to Nogier, the different zones are assigned to different functional areas:
| Entodermal zone |
|
| Mesodermal zone |
|
| Ectodermal zone |
|
 Metabolism, organs
Metabolism, organs Motor system
Motor system Head and central nervous system
Head and central nervous systemIn line with this tripartition, Nogier found one control point for each functional area; these are the Omega Points.
 Auriculotemporal nerve
Auriculotemporal nerve
(trigeminal nerve)
 Auricular branch
Auricular branch
(vagus nerve)
 Great auricular nerve
Great auricular nerve
(cervical plexus)
Zones of Auricular Innervation According to Nogier

Zones of Auricular Innervation According to R.A. Durinjan
The description of the auricular zones of innervation and the various somatopic representations according to the Russian school goes back to R.A. Durinjan. The first comprehensive German-language presentation of Russian auriculotherapy came from R. Umlauf and was published in 1988 in the German Journal of Acupuncture (Deutsche Zeitschrift für Akupunktur).
According to Durinjan, the following five nerves participate in the innervation of the auricula:
 Fibers of the cervical plexus
Fibers of the cervical plexus
 The trigeminal nerve,
The trigeminal nerve,
 The intermediate nerve of the facial nerve,
The intermediate nerve of the facial nerve,
 The glossopharyngeal nerve,
The glossopharyngeal nerve,
 The auricular branch of the vagus nerve.
The auricular branch of the vagus nerve.
The innervation zones show distinct overlaps of all the areas innervated by the five participating nerves. No auricular zone is therefore exclusively innervated by one single nerve. This might explain why two or more acupuncture points of different functions are projected on identical anatomical sites. Likewise, projections of the same organ are ascribed to different sites of localization. For example, we find projections which correspond to the parenchyma of the organ, next to them projections of the corresponding nervous innervation, and, finally, projections representing the functional state of the organ. Due to the variation in auricular shape, it is conceivable that the overlaps of innervation zones also vary individually. Thus, the frequently described points are really zones rather than points in which the actual ear acupuncture point must be searched for according to individual circumstances. No doubt, this approach goes back to Nogier, who tried to find individual representations of acupuncture points by means of the auriculocardiac reflex (ACR) (cf. p. 30).

Cervical plexus

Glossopharyngeal nerve

Intermediate nerve (facial nerve)

Trigeminal nerve

Vagus nerve
More Recent Investigations into Auricular Innervation
More recent investigations into auricular innervation (Peuker and Filler, 2001) verify a very high density and number of nerve fibers on the external ear compared to other regions of the head. Supply is via four different nerves of both branchiogenic and somatogenic origin:
 The great auricular nerve (cervical plexus)
The great auricular nerve (cervical plexus)
 The auriculotemporal nerve (trigeminalnerve)
The auriculotemporal nerve (trigeminalnerve)
 The auricular branch of the vagus nerve
The auricular branch of the vagus nerve
 The occipitalis minor nerve (cervical plexus).
The occipitalis minor nerve (cervical plexus).
With regard to sensitive innervation, there is a gap between the beginning of the first and third branchiogenic nerve and the third to fifth spinal nerve. There is no overlap between the brianchial arch nerves although there is between the somatogenic nerves and with the brianchial arch nerves.
On the lateral surface, supply via the great auricular nerve (cervical plexus) dominates. The anthelix is mainly supplied solely by the auricular branch of the vagus nerve, in part, by the great auricular nerve, or by both together. The anthelical crura are predominantly innervated by the great auricular nerve. The lobulus and antitragus are usually innervated by the great auricular nerve.
The tragus is mainly supplied jointly by the great auricular nerve and the auriculotemporal nerve. The tail of the helix and scapha are almost always supplied solely by the great auricular nerve; the spina helicis approximately 90% by the auriculotemporal nerve.
The cymba concha is constantly innervated by the auricular branch of the vagus nerve, the cavity of the inferior concha in approximately 50% of cases. In the other 59% of cases, there is dual innervation with the great auricular nerve. There is no overlapping of the zones of innervation of three nerves in any area.
On the dorsal side, the occipitalis minor nerve is involved in innervation, in the upper third often together with the great auricular nerve.
The great auricular nerve and the auricular branch of the vagus nerve are involved in the supply of the middle third, less often the occipitalis minor nerve. The great auricular nerve almost always innervates the lower third, less often the auricular branch of the vagus nerve. There is no area on the dorsal side with threefold innervation either.
Various studies suggest that sensitive innervation of the auricula takes place by means of cranial and cervical nerves (Satomi and Takahashi, 1991). There is still no conclusive explanation for the function of such extensive innervation in man. Possibly, temperature regulation and control of the formation of the ear plays a part here.
Anatomical manuals and atlases examine the nerve supply of the auriculain surprisingly little detail. Most auricular acupuncture manuals are more detailed in this area. However, assumptions with little scientific basis appear to be handed down fromone work to another with regard to the areas of innervation, possibly because in this way hypotheses about postulated modes of action can be supported. An excellent example here is the distinction between entodermal, mesodermal, and ectodermal innervation areas (see above) which cannot be defended for various reasons

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


