Chapter 34 Atherosclerosis



Morphology
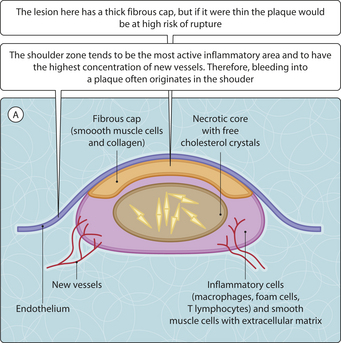
The earliest visible lesion is the fatty streak, a slightly raised yellow spot or band within the intima. These lesions can develop into an atheromatous plaque, which has a soft yellow core covered by a fibrous cap (Fig. 3.34.1). The word atherosclerosis reflects the consistency of the plaques: the soft, lipid-rich core (from the Greek word for porridge, athere) and the fibrous sclerotic part. The core consists of necrotic tissue, collections of cholesterol and other lipids, and foam cells containing ingested lipid. Although most of the foam cells are macrophages that derive from blood monocytes, there is evidence that smooth muscle cells can also become phagocytic and transform into foam cells. Around the necrotic core, proliferating smooth muscle cells, macrophages and T-lymphocytes are found. Some lesions also include other inflammatory cells, and chronic inflammation can be important in weakening the plaque or the underlying media. Collagen and other intercellular matrix components are produced by the smooth muscle cells, which act as if they have some characteristics of fibroblasts.
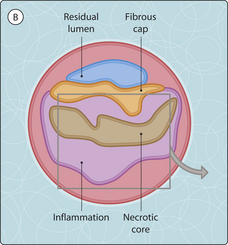
Plaques may undergo a number of changes, in which case they are said to be complicated (Table 3.34.1). Some of these complications have serious sequelae. Stenosis or occlusion of an artery can follow either thrombosis of an ulcerated plaque or haemorrhage into a plaque, with subsequent ischaemia or infarction of the tissue supplied by the artery. Some conditions predispose to the development of critical ischaemia when the normal passage of blood through an artery is prevented:
 reduced oxygen-carrying capacity of the blood, caused either by a low haemoglobin concentration (anaemia) or by irreversible combination of haemoglobin with a substance other than oxygen (e.g. carbon monoxide, which produces carboxyhaemoglobinaemia)
reduced oxygen-carrying capacity of the blood, caused either by a low haemoglobin concentration (anaemia) or by irreversible combination of haemoglobin with a substance other than oxygen (e.g. carbon monoxide, which produces carboxyhaemoglobinaemia)



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


