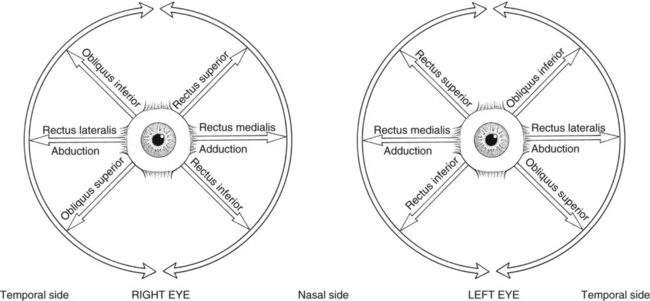
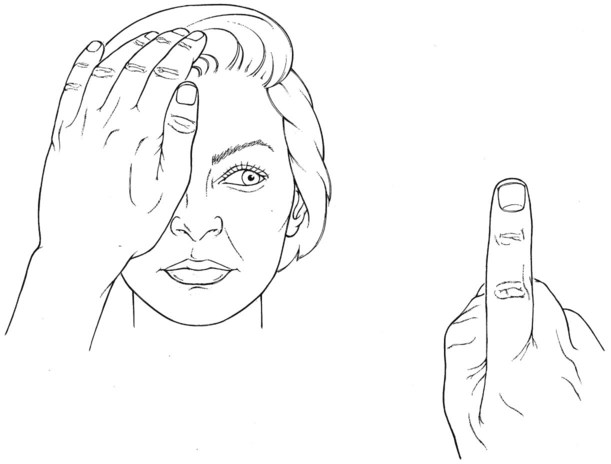
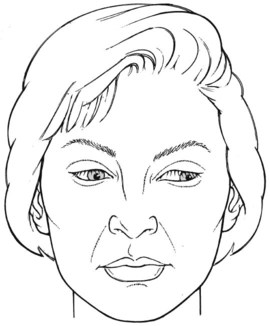
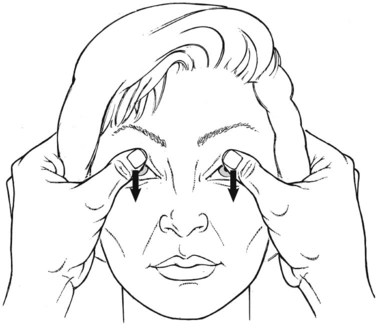
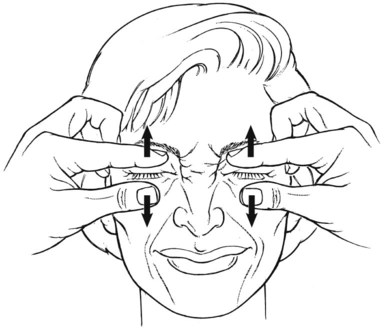
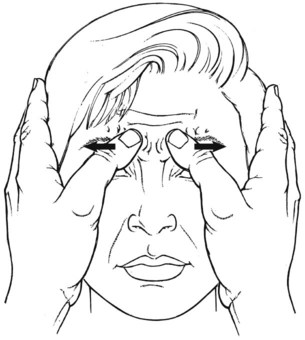
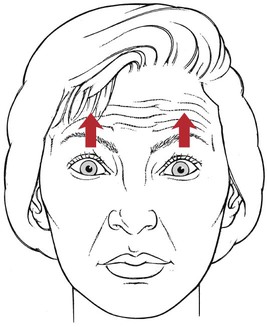
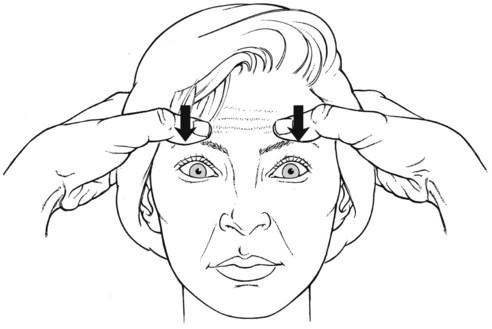
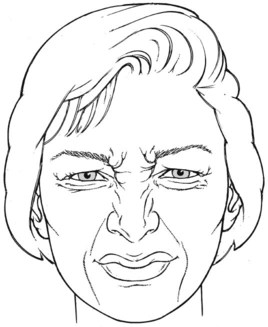
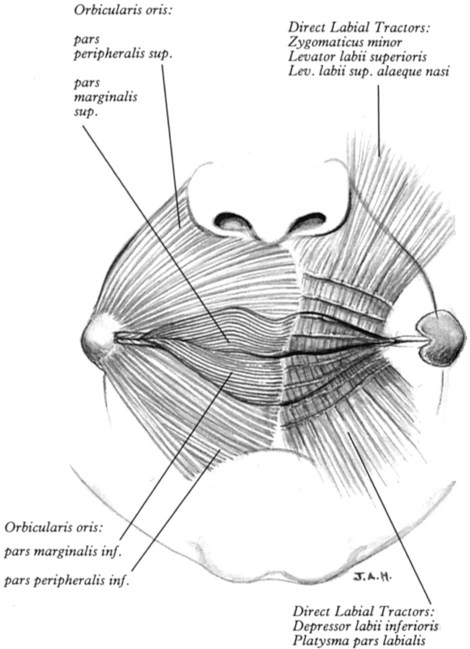
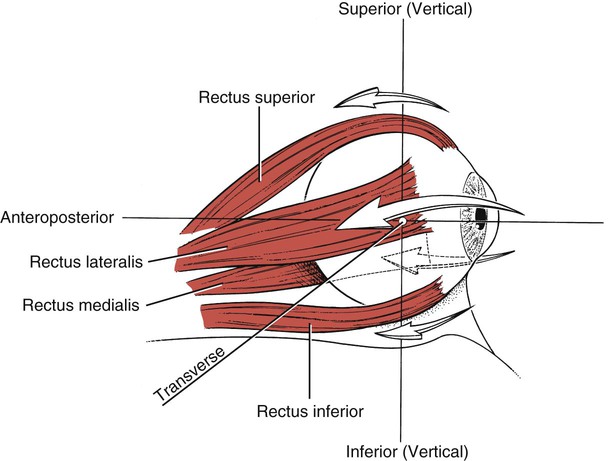
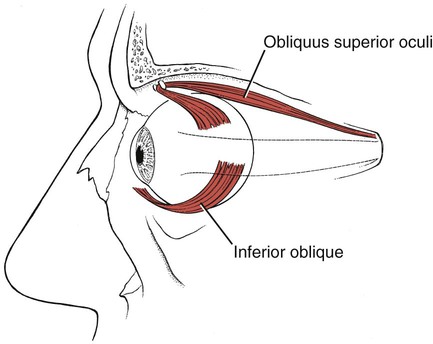
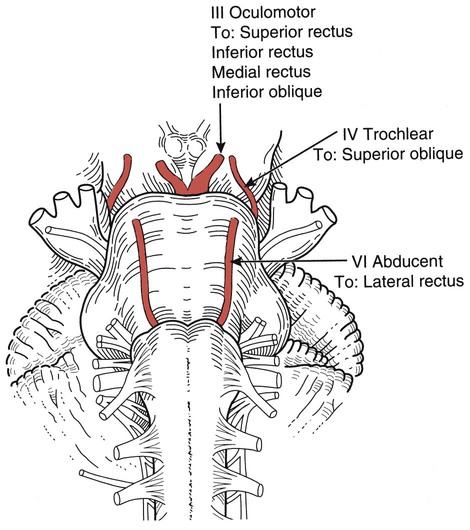
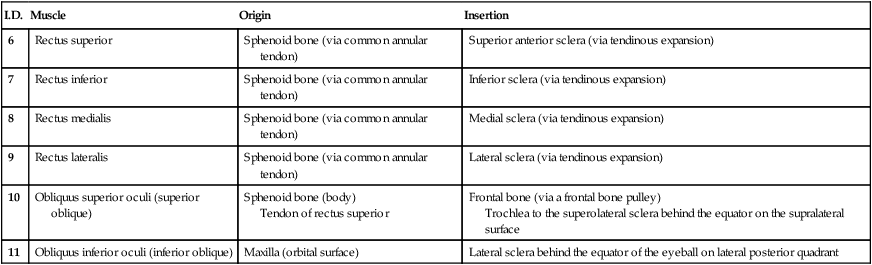
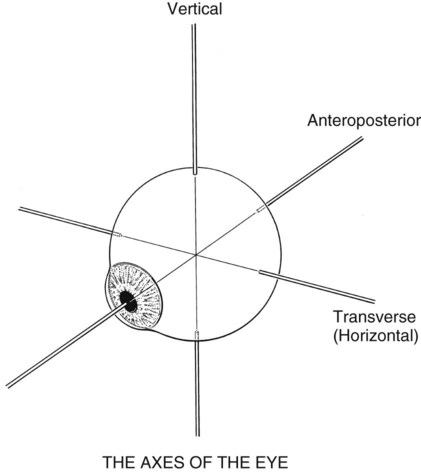
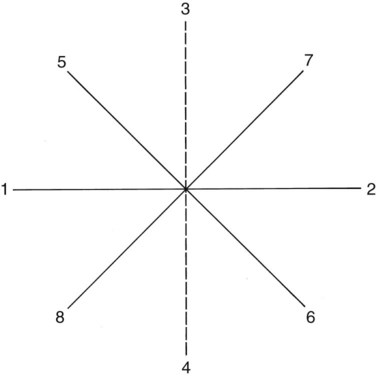
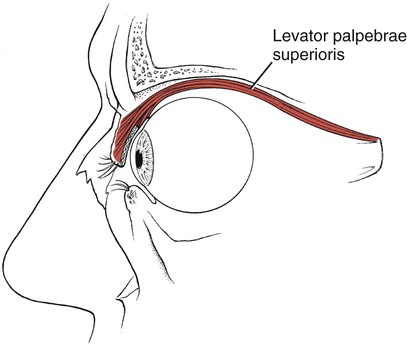
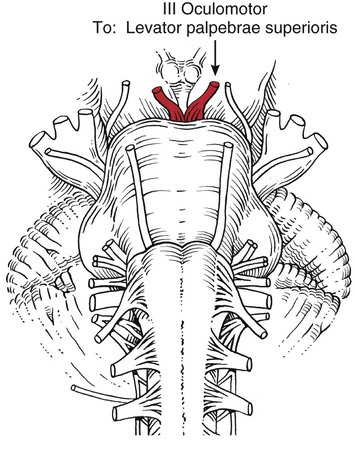
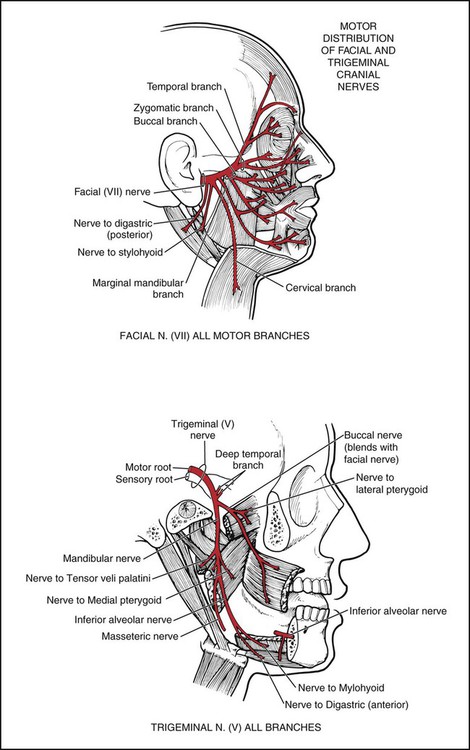
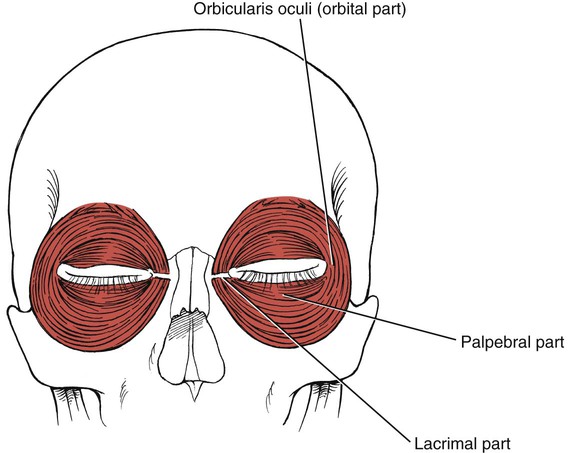
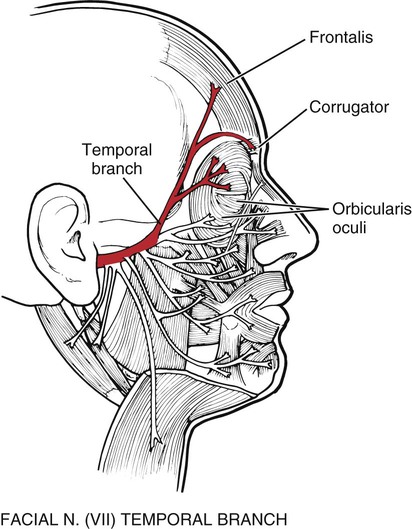
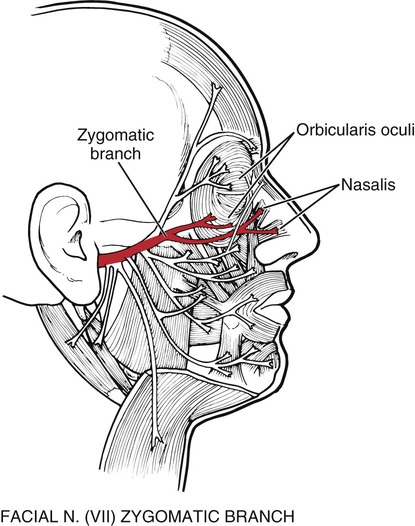
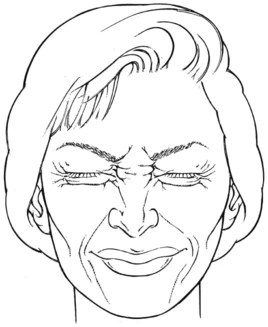
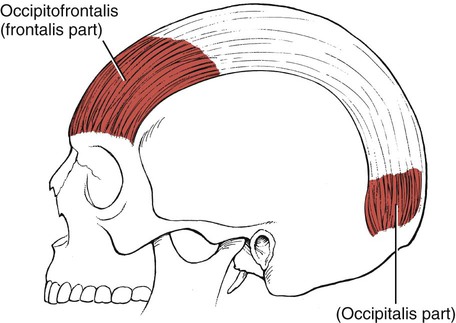
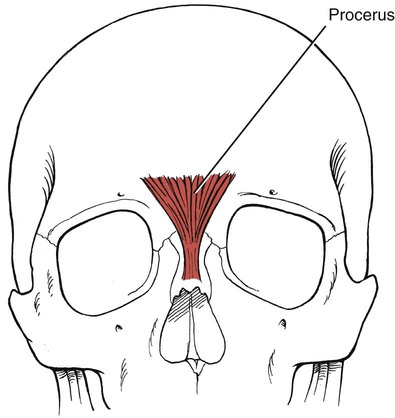
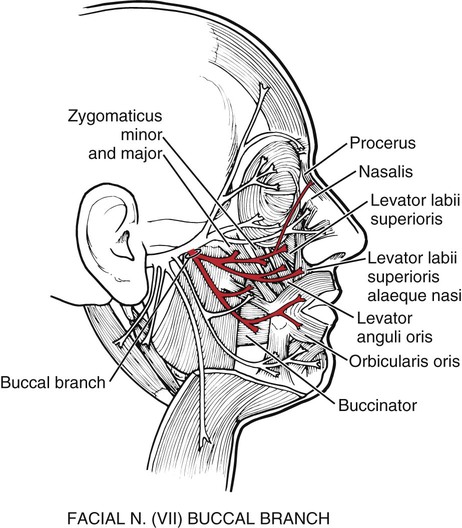
The six extraocular muscles of the eye (Figure 7-1 and Figure 7-2) move the eyeball in directions that depend on their attachments and on the influence of the movements themselves. It is usual that no muscle of the eye acts independently, and because these muscles cannot be observed, palpated, or tested individually, much of the knowledge of their function is derived from some variety of dysfunction. The extraocular muscles are innervated by cranial nerves III (oculomotor), IV (trochlear), and VI (abducent) (Figure 7-3). Table 7-1 The eyeball rotates in the orbital socket around one or more of three primary axes (Figure 7-4), which intersect in the center of the eyeball.1 Vertical axis: Around this axis the lateral motions (abduction and adduction) take place in a horizontal plane. Transverse axis: This is the axis of rotation for upward and downward motions. Anteroposterior axis: Motions of rotation in the frontal plane occur around this axis. The extraocular muscles seem to work as a continuum; as the length of one changes, the length and tension of the others are altered, giving rise to a wide repertoire of paired movements.2,3 Despite this continuous commonality of activity, the function of the individual muscles can be simplified and understood in a manner that does not detract from accuracy but simplifies the test procedure. Conventional clinical testing assigns the following motions to the various extraocular muscles (Figure 7-5).1–3 2. Rotation of the eyeball so the vertical axis is outward. 3. Note: In paralysis, the eyeball is deviated downward and somewhat laterally; it cannot move upward when in abduction. 4. Note: In a III nerve lesion, the eye is outward and cannot be brought in. This lesion also results in ptosis, or drooping, of the upper eyelid.2,3 Eye movements are tested by having the patient look in the cardinal directions (numbers in parentheses refer to tracks shown in Figure 7-6).2 All pairs in tracking are antagonists. Laterally (1) Upward and laterally (5) Medially (2) Upward and medially (7) Upward (3) Downward and medially (6) Downward (4) Downward and laterally (8) The range, speed, and smoothness of the motion should be observed, as well as the ability to sustain lateral and vertical gaze.2–4 The therapist will not be able to use these observational methods to distinguish movement deviations accurately because accuracy requires the sophisticated instrumentation used in ophthalmology. The tracking movements will appear normal or abnormal, but little else will be possible. Table 7-2 MUSCLES OF THE EYELIDS AND EYEBROWS The face should be observed for mobility of expression, and any asymmetry or inadequacy of muscles should be documented. A one-sided appearance when talking or smiling, a lack of tone (with or without atrophy), the presence of fasciculations, asymmetrical or frequent blinking, smoothness of the face, or excessive wrinkling are all clues to VII nerve involvement. Opening the eye by raising the upper eyelid is a function of the levator palpebrae superioris (see Figure 7-10). The muscle should be evaluated by having the patient open and close the eye with and without resistance. The function of this muscle is assessed by its strength in maintaining a fully opened eye against resistance. In the presence of a facial (VII) nerve lesion, the levator sign may be present.2 In this case, the patient is asked to look downward and then slowly close the eyes. A positive levator sign is noted when the upper eyelid on the weak side moves upward because the action of the levator palpebrae superioris is unopposed by the orbicularis oculi. Involvement of the facial nerve may result from a lesion that affects the nerve or the nucleus (i.e., a peripheral lesion). Motor functions of the face also may be impaired after a central or supranuclear lesion. These two sites of interruption of the VII nerve lead to dissimilar clinical problems.5 The orbicularis oculi muscle is the sphincter of the eye (Figure 7-13).1 Its lids are innervated by the facial (VII) nerve (temporal branch and zygomatic branch) (Figures 7-14 and 7-15). Its palpebral portion closes the eyelids gently, as in blinking and sleep. The orbital portion of the muscle closes the eyes with greater force, as in winking. The lacrimal portion draws the eyelids laterally and compresses them against the sclera to receive tears. All portions act to close the eyes tightly (Figure 7-16). Observation of the patient without specific testing will detect weakness of the orbicularis because the blink will be delayed on the involved side. To examine the frontal belly of the occipitofrontalis muscle (Figure 7-21 and see Figure 7-14), the patient is asked to create an expression of surprise where the forehead skin wrinkles horizontally. The occipital belly of the muscle is not tested usually, but it draws the scalp backward. Table 7-3 *The depressor septi often is considered part of the dilator nares. The three muscles of the nose are all innervated by the facial (VII) nerve. The procerus (Figure 7-24) draws the medial angle of the eyebrows downward, causing transverse wrinkles across the bridge of the nose. The nasalis (compressor nares) depresses the cartilaginous portion of the nose and draws the ala down toward the septum (see Figure 7-15). The nasalis (dilator nares) dilates the nostrils. The depressor septi draws the alae downward, constricting the nostrils. Table 7-4 One major source of confusion is the relationship between the muscles around the mouth. The common description until recently was of uninterrupted circumoral muscles. In fact, the orbicularis oris muscle is not a complete ellipse but rather contains fibers from the major extrinsic muscles that converge on the buccal angle, as well as intrinsic fibers.1,6,7 The authors and others do not describe complete ellipses, but most drawings illustrate such.6 The area on the face that has a large concentration of converging and diverging fibers from multiple directions lies immediately lateral and slightly above the corner of the mouth. Using the thumb and index finger on the outer skin and inside the mouth and compressing the tissue between them will quickly identify the knotlike structure known as the modiolus.8–10 The modiolus (from the Latin meaning nave of a wheel) is described as a muscular or tendinous node, a rather concentrated attachment of many muscles.8,9 Its basic shape is conical (though this is oversimplified); it is about 1 cm thick and is found in most people about 1 cm lateral to the buccal angle. Its shape and size vary considerably with gender, race, and age. The muscular fibers enter and exit on different planes, superficial and deep, with some spiraling, but essentially they constitute a three-dimensional complexity. Different classifications of modiolar muscles exist, but basically 9 or 10 facial muscles are associated with the structure:9 When the modiolus is firmly fixed, the buccinator can contract to apply force to the cheek teeth; the orbicularis oris can contract against the arch of the anterior teeth, thus sealing the lips together and closing the mouth tightly.9 Similarly, control of the modiolar active and stay muscles enables accurate and fine control of lip movements and pressures in speech. This circumoral muscle (Figures 7-28 and 7-29) serves many functions for the mouth. It closes the lips, protrudes the lips, and holds the lips tight against the teeth. Furthermore, it shapes the lips for such functional uses as kissing, whistling, sucking, drinking, and the infinite shaping for articulation in speech. (For innervation, see Figure 7-25.)
Assessment of Muscles Innervated by Cranial Nerves
Jacqueline Montgomery
Introduction to Testing and Grading
Extraocular Muscles
I.D.
Muscle
Origin
Insertion
6
Rectus superior
Sphenoid bone (via common annular tendon)
Superior anterior sclera (via tendinous expansion)
7
Rectus inferior
Sphenoid bone (via common annular tendon)
Inferior sclera (via tendinous expansion)
8
Rectus medialis
Sphenoid bone (via common annular tendon)
Medial sclera (via tendinous expansion)
9
Rectus lateralis
Sphenoid bone (via common annular tendon)
Lateral sclera (via tendinous expansion)
10
Obliquus superior oculi (superior oblique)
Sphenoid bone (body)
Tendon of rectus superior
Frontal bone (via a frontal bone pulley)
Trochlea to the superolateral sclera behind the equator on the supralateral surface
11
Obliquus inferior oculi (inferior oblique)
Maxilla (orbital surface)
Lateral sclera behind the equator of the eyeball on lateral posterior quadrant
The Axes of Eye Motion
Eye Motions
11 Obliquus inferior (III, Oculomotor)
Eye Tracking
Muscles of the Face and Eyelids
I.D.
Muscle
Origin
Insertion
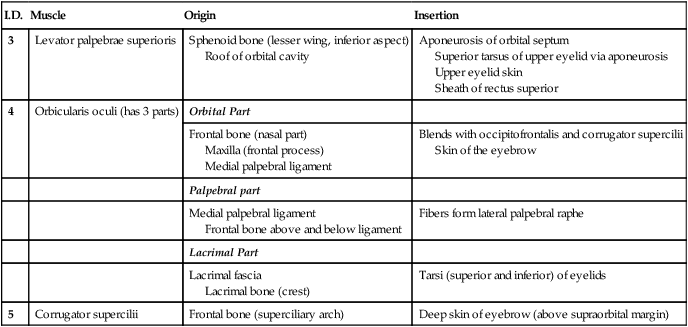
3
Levator palpebrae superioris
Sphenoid bone (lesser wing, inferior aspect)
Roof of orbital cavity
Aponeurosis of orbital septum
Superior tarsus of upper eyelid via aponeurosis
Upper eyelid skin
Sheath of rectus superior
4
Orbicularis oculi (has 3 parts)
Orbital Part
Frontal bone (nasal part)
Maxilla (frontal process)
Medial palpebral ligament
Blends with occipitofrontalis and corrugator supercilii
Skin of the eyebrow
Palpebral part
Medial palpebral ligament
Frontal bone above and below ligament
Fibers form lateral palpebral raphe
Lacrimal Part
Lacrimal fascia
Lacrimal bone (crest)
Tarsi (superior and inferior) of eyelids
5
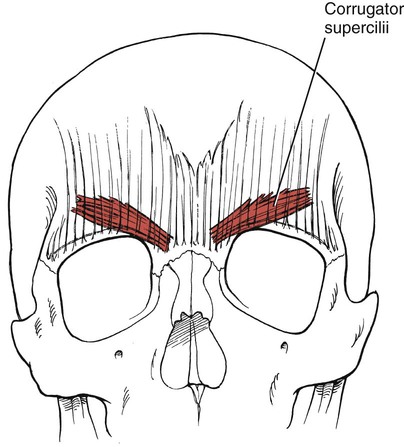
Corrugator supercilii
Frontal bone (superciliary arch)
Deep skin of eyebrow (above supraorbital margin)
Eye Opening (3. Levator palpebrae superioris)
Criteria for Grading
 Peripheral versus Central Lesions of the Facial (VII) Nerve
Peripheral versus Central Lesions of the Facial (VII) Nerve
Closing the Eye (4. Orbicularis oculi)
Raising the Eyebrows (1. Occipitofrontalis, frontalis part)
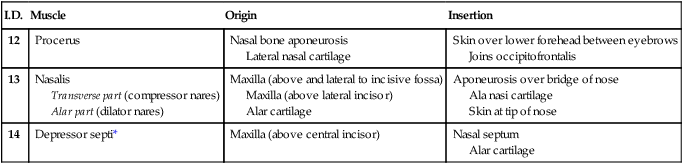
Nose Muscles
I.D.
Muscle
Origin
Insertion
12
Procerus
Nasal bone aponeurosis
Lateral nasal cartilage
Skin over lower forehead between eyebrows
Joins occipitofrontalis
13
Nasalis
Transverse part (compressor nares)
Alar part (dilator nares)
Maxilla (above and lateral to incisive fossa)
Maxilla (above lateral incisor)
Alar cartilage
Aponeurosis over bridge of nose
Ala nasi cartilage
Skin at tip of nose
14
Depressor septi*
Maxilla (above central incisor)
Nasal septum
Alar cartilage
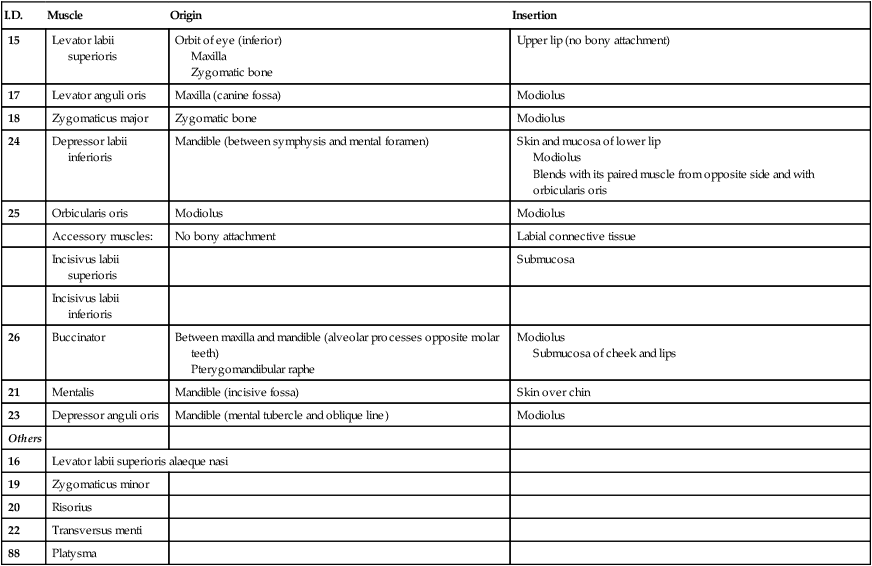
Muscles of the Mouth and Face
I.D.
Muscle
Origin
Insertion
15
Levator labii superioris
Orbit of eye (inferior)
Maxilla
Zygomatic bone
Upper lip (no bony attachment)
17
Levator anguli oris
Maxilla (canine fossa)
Modiolus
18
Zygomaticus major
Zygomatic bone
Modiolus
24
Depressor labii inferioris
Mandible (between symphysis and mental foramen)
Skin and mucosa of lower lip
Modiolus
Blends with its paired muscle from opposite side and with orbicularis oris
25
Orbicularis oris
Modiolus
Modiolus
Accessory muscles:
No bony attachment
Labial connective tissue
Incisivus labii superioris
Submucosa
Incisivus labii inferioris
26
Buccinator
Between maxilla and mandible (alveolar processes opposite molar teeth)
Pterygomandibular raphe
Modiolus
Submucosa of cheek and lips
21
Mentalis
Mandible (incisive fossa)
Skin over chin
23
Depressor anguli oris
Mandible (mental tubercle and oblique line)
Modiolus
Others
16
Levator labii superioris alaeque nasi
19
Zygomaticus minor
20
Risorius
22
Transversus menti
88
Platysma
 The Modiolus
The Modiolus
Levator anguli oris
Levator labii superioris
Orbicularis oris
Levator labii superioris alaeque nasi
Depressor anguli oris
Zygomaticus minor
Zygomaticus major
Mentalis
Depressor labii inferioris
Buccinator
Lip Closing (25. Orbicularis oris)