Chapter 2 Assessment of Disease Activity in Systemic Lupus Erythematosus
Systemic lupus erythematosus (SLE) is a complex disease characterized by the occurrence of various clinical manifestations that can be related to acute disease activity or chronic damage. The distinction between active, potentially treatable manifestations and permanent damage is critical in routine clinical practice. Assessment of disease activity in SLE patients is a problem faced every day by treating physicians.
The simplest disease activity scale in use is an analogue global assessment scale1,2 that consists of a line (usually 10 cm) along which the rater draws a perpendicular mark, reflecting his or her overall judgment of disease activity (far left usually indicates no disease activity, and far right the most severe). This allows for a fairly reliable indicator of the rater’s overall impression after factoring in the entire complexity of subjective and objective signs suggesting individual organ activity, worsening, or improvement. Although generally considered as the “gold standard” for disease activity, this scale has great inter- as well as intra-rater variability.2–5 This feature becomes problematic when the assessment of activity in many patients is required in clinical research or in drug efficacy trials. However, given the heterogeneity of signs and symptoms related to systemic lupus and the unpredictable fluctuations of the disease, the development of reliable and reproducible disease activity indices that can outperform the simple analogue scale has not been easy.
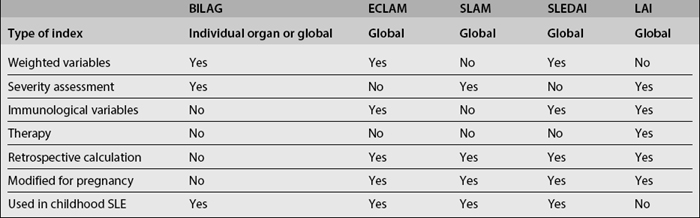
The evolution of valid and sensitive methods to assess disease activity has progressed slowly in the past 25 years. Some indices such as the BILAG, ECLAM, SLAM, SLEDAI and LAI (Table 2.1) have been validated in prospective studies,6–8 and their reproducibility, validity, and sensitivity to change have been compared.8 These instruments are now widely used in clinical research, including randomized controlledtrials of investigational treatments, with varying degrees of success. Critical factors in the use of formulated disease activity indices in multicenter studies of lupus are investigator training and consensus among investigators about how these instruments should be applied. Equally important is to understand from the beginning the strengths and limitations of each instrument so that each is applied along with an optimal study design.
Most activity measures are useful mainly as scoring systems for overall (global) disease activity (ECLAM, SLAM, SLEDAI, LAI). Global scores are useful to compare variables or interventions that apply widely across entire cohorts of SLE patients, since they allow comparisons of patients with a variety of disease manifestations. Global indices may also be used to provide benchmarks to define criteria for entry in some clinical trials. However, a global score does not differentiate between modest activity in many organs and high activity in one single organ, and may tend to blur the line between prognostic categories. The BILAG instrument was designed to provide separate scores for individual organ systems but can be used as a global disease measure. Assessment of individual organs allows quantification of the number or organs involved, the variable severity with which each organ might be affected, and, the ability to sort large cohorts into prognostic or therapeutic subgroups.3–5 The most widely used activity indices in SLE are reviewed below.
BRITISH ISLES LUPUS ASSESSMENT GROUP INDEX
First reported in 1988,6 scoring of the BILAG is anchored in the physician’s intention to treat and assesses overall disease activity during the month previous to examination in each of eight organ systems: general, mucocutaneous, neurological, musculoskeletal, cardiovascular/respiratory, renal, and hematological.6,7 Laboratory and diagnostic testing required at each visit are relatively simple and usually ordered in routine clinical practice. However, when clinically indicated, more sophisticated testing can provide diagnostic data that reflect on the BILAG score. These aspects allow the calculation of the index with minimal expense and potentially in any clinical setting, but ensures that for very sick patients scoring can be made as accurate as possible.
Activity in each organ system is scored as follows: A, most active disease; B, intermediate activity; C, mild, stable disease; D, inactive disease in a previously affected organ; and E, no history of any activity. These scores are derived from assessment of a number of potential clinical manifestations in each organ system as to whether during the past month each has been absent, new, getting worse, getting better, or remaining overall the same as in the previous month. Manifestations are further weighted by assigning more impact to severe forms of each disorder (e.g., polyarticular arthritis with loss of function receives an A score, and so is weighted to score more heavily than simple arthritis, which engenders a B score) (see Appendix E). By assigning numerical values to the activity scores for each organ system, (A=9, B=3, C=1, D or E=0) it is possible to calculate a global activity score ranging from 0 to 72 (albeit in practice scores as high as 27 are rare). The reliability, validity, and sensitivity to change of the BILAG have been evaluated both by the original study group and independent investigators.7–11 The index was reviewed in 2000 and in 2004.12,13 In the last version, two additional systems—gastrointestinal and ophthalmic—were added (see Appendices G, H, and I). In 2004 the validity of the BILAG in assessing disease activity in childhood onset SLE was also demontrated.14
The BILAG index can be calculated with a computerized program, the British Lupus Integrated Prospective System (BLIPS). This software can calculate, along with the BILAG index, SLAM, SLEDAI, SLICC/ACR Damage Index, and SF-36 patient Health Questionnaire.12
EUROPEAN CONSENSUS LUPUS ACTIVITY MEASUREMENT
The ECLAM index is the result of work done between 1990 and 1992 by a European Consensus Study Group aimed at defining disease activity in SLE, distinguishing clinical and serological variables that most identify disease activity, and comparing disease activity scales.15–18
A standardized clinical chart was prepared to record data from consecutively observed SLE patients, and the physician global assessment (PGA) was considered as the reference “gold standard” for lupus activity. Data from 704 SLE patients from various European centers were obtained and examined. Univariate analysis was performed to select the symptoms and laboratory parameters that best predicted disease activity. Multivariate regression analyses were carried out to define the relative weight of each variable. Therefore, the ECLAM derives from the study of real patients.15–18
The index, a global activity score, assesses disease activity within the past month. It comprises 15 weighted clinical and serological items, and scores disease activity from 0 to 10 (see Appendix J). Autoantibody testing is not included in the index, and the serological variables required to calculate the ECLAM (ESR, blood count, serum creatinine, urine analysis, and complement levels) are those normally used in routine clinical practice, facilitating its use in any clinical setting and at any patient’s visit.15
The reliability, validity, and sensitivity to change of the ECLAM have been evaluated both by the original study group who designed the index as well as by independent investigators.10,17–19 In 2000 the ECLAM index was validated for the retrospective calculation of disease activity from the data provided in patients’ clinical charts. The instrument’s reliability is good depending on the quality of data recorded on clinical charts.20
The ECLAM has been validated for use in pediatric lupus, and recently the Pediatric Rheumatology International Trials Organization (PRINTO) included the ECLAM in a disease activity core set21,22 to be used in clinical trials in juvenile SLE. A modified version for use in pregnancy exists.23
After training, 5 minutes are required to complete the ECLAM, which makes the index very easy to be used in routine clinical settings. A computerized program (ACTICARD) is also available to record patient demographic and clinical data, collect all variables that contribute to the assessment of disease activity, and automatically calculate at each visit the most used activity indices in SLE (ECLAM, SLAM, SLEDAI). The computerized program requires 10 minutes to complete, and validity of ACTICARD in the retrospective calculation of the ECLAM index has been evaluated.24
Related posts:
 Biomarkers of Disease Activity
Biomarkers of Disease Activity
 Antibodies and their Antigenic Targets in the Antiphospholipid Syndrome
Antibodies and their Antigenic Targets in the Antiphospholipid Syndrome
 Overview of the Pathogenesis of Systemic Lupus Erythematosus
Overview of the Pathogenesis of Systemic Lupus Erythematosus
 Complement Deficiencies in Human Systemic Lupus Erythematosus (SLE) and SLE Nephritis: Epidemiology and Pathogenesis
Complement Deficiencies in Human Systemic Lupus Erythematosus (SLE) and SLE Nephritis: Epidemiology and Pathogenesis
 What Do Mouse Models Teach Us about Human Systemic Lupus Erythematosus?
What Do Mouse Models Teach Us about Human Systemic Lupus Erythematosus?
 Infection and Autoimmunity
Infection and Autoimmunity



