Fig. 16.1
Fluoroscopic (a) and arthroscopic (b) imaging of the wrist during the excision of the scaphoid
With the arthroscope in the ulnar viewing (MCU) portal, the scaphoid is excised with the bur, moving from ulnar to radial, and distal to proximal. The bur is then typically placed more radially in the STT portal to remove the distal pole of the scaphoid. Under direct arthroscopic visualization, a fine synovial rongeur is useful to remove small fragments of bone or cartilage that remain adherent to capsule (Fig. 16.2). Complete excision of the distal pole of the scaphoid is left to the discretion of the surgeon (Fig. 16.3).
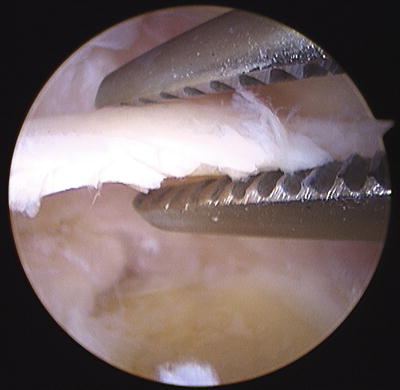

Fig. 16.2
Arthroscopic imaging of bone fragment excision using a fine synovial rongeur
Fig. 16.3
A fluoroscopic image of the wrist following the scaphoid excision
Following scaphoid excision, the arthroscope is then placed in the STT portal. With the arthroscope placed radially, and viewing ulnarly, the bur is placed in an enlarged MCR portal. The lunate is then excised with the bur, now working radial to ulnar, and distal to proximal (Fig. 16.4). Great care should be taken when removing the proximal layer of articular cartilage of the lunate, but traction usually creates a safe space above the distal radius. Again, the use of fine synovial rongeurs facilitates removal of small fragments of bone and cartilage that remain adherent to the capsule. Following removal of the lunate, the arthroscope is moved to the MCR portal, the bur is placed in the MCU portal, and the triquetrum is excised. Confirmation of a complete APRC is made with fluoroscopy (Fig. 16.5).
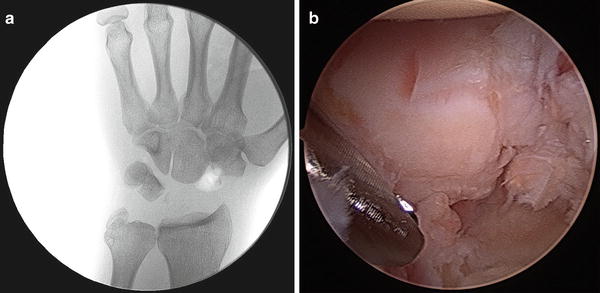
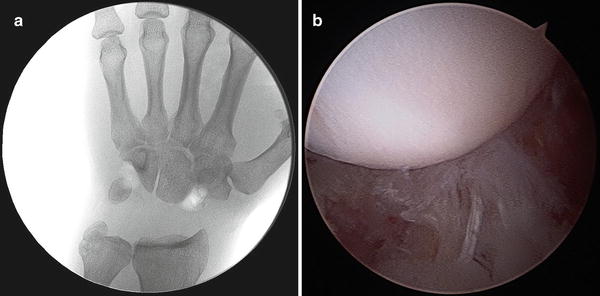
Fig. 16.4
Fluoroscopic (a) and arthroscopic (b) imaging of the wrist following removal of the lunate
Fig. 16.5
Fluoroscopic (a) and arthroscopic (b) imaging of the wrist following complete arthroscopic proximal row carpectomy while the wrist is in traction
The limb is then taken out of traction, and the radiocapitate joint is reduced. Seating of the head of the capitate in the lunate fossa of the radius is confirmed both arthroscopically and with fluoroscopy (Fig. 16.6). Range of motion of the wrist under fluoroscopy will confirm stability, and also reveal occasional radial styloid impingement, which can be treated with arthroscopic radial styloidectomy (performed with the bur in the 1/2 portal).
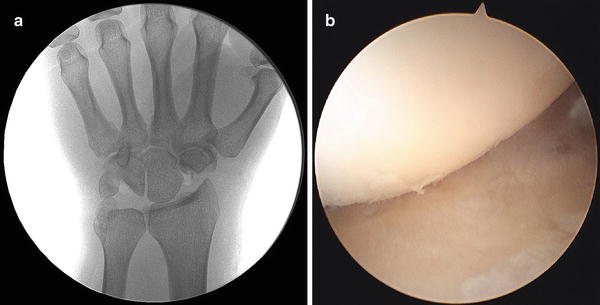
Fig. 16.6
Fluoroscopic (a) and arthroscopic (b) imaging of the newly formed wrist joint after the wrist is released from traction
Postoperatively, the wrist is injected with bupivacaine, and a bulky dressing and volar splint are applied, allowing for immediate finger range of motion. The patient is seen in the office 2 days postoperatively, when the bandage is removed, and a removable volar splint is applied for comfort. Early active and passive range of motion of the wrist is encouraged, and return to activity is within the limits of patient comfort. Formal hand therapy is prescribed on an individual basis as needed.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


