Stage 1
Normal radiographs. Signal intensity changes on MRI scan
Stage 2
Sclerosis of the lunate on radiographs; Fracture lines may be seen, but no collapse
Stage 3
Collapse of the lunate articular surface.
Stage 3A
Normal carpal alignment and height.
Stage 3B
Abnormal carpal alignment. Fixed scaphoid rotation, proximal capitate migration, and loss of carpal height.
Stage 4
Collapse of the lunate associated with radiocarpal or midcarpal arthritis
Arthroscopy provides direct visualization of the articular cartilage and allows assessment of the radiocarpal and midcarpal joints. The disparity between radiographic and arthroscopic assessment has been highlighted by Ribak, who reported that plain radiographs correlated poorly with arthroscopic findings [6]. This was reinforced by Bain and Begg, who reported that it was not uncommon for plain radiographs to underscore the severity of the articular involvement identified with arthroscopy [7].
The Role of Wrist Arthroscopy
In 1999 Menth-Chiari et al. first described the use of wrist arthroscopy for the treatment of Kienböck’s disease [8]. Their model was to use arthroscopy to assess the articular surfaces, to debride the necrotic lunate and perform a limited synovectomy. In their study all patients were either Lichtman grade IIIA or IIIB, and all experienced relief of their painful mechanical symptoms.
Wrist arthroscopy has become a valuable assessment and primary treatment tool in the treatment of Kienböck’s disease. The authors use arthroscopy to perform the initial debridement and to identify the nonfunctional joints to tailor the surgical reconstruction to the anatomic findings [7]. This system uses direct visual assessment of the articulations of the lunate and a probe to assess the degree of softening of the articular surfaces. Correlating this arthroscopic assessment with traditional investigations helps the clinician make better-informed management decisions. The advantage is that functional joint surfaces determine treatment.
Arthroscopic Technique
Wrist arthroscopy is performed using the standard technique. The patient is placed supine with their arm on an arm board. A tourniquet is used. Traction is applied from a tower mounted on the opposite side of the bed, and the arm is suspended using finger traps. A counter traction weight of 4 kg is attached to a sling and draped over the tourniquet on the patient’s upper arm. Standard 3/4, 6R and midcarpal portals are used.
The articular surface of the lunate is examined from the radiocarpal and the midcarpal joint. The articular surface is probed. If there is a subchondral fracture, then the cartilage will be soft, indicating a floating articular surface. The articular surfaces of the lunate facet of the distal radius and the head of the capitate are also inspected and probed. Fracture of the lunate may be identified and any loose bodies are removed. Synovitis is identified. If no further surgery is planned the joint is debrided.
Pathological Phases of Kienböck’s Disease
Avascular necrosis of the lunate consists of three pathological phases: vascular (early), osseous (intermediate), and chondral (late) [9] (Fig. 20.1).
Fig. 20.1
The pathological phases of Kienböck’s disease showing the association between the vascular, osseous, and chondral phases [Reprinted from Bain GI, Durrant A. An articular-based approach to Kienböck avascular necrosis of the lunate. Tech Hand Up Extrem Surg. 2011;15(1):41–7. With permission Wolters Kluwer Health]
Early Vascular
Changes in the lunate commence with ischemia, subsequent necrosis and revascularization. MRI and bone scan are of value in interpreting the vascular changes.
Intermediate Osseous
Lichtman has described this phase well over the last 36 years. CT scan is of value and it demonstrates well the detail of the osseous changes [10]. The initial radiological changes are of sclerosis, followed by subchondral collapse. Multiple faults or plates occur in the trabeculae and when the formation of these outstrips the repair, the blood supply may be disrupted and result in bone necrosis [11]. It has been shown that the trabecular structure of lunates affected by Kienböck’s disease is different from that of normal lunates. The trabeculations are denser and thicker, whereas the surface area and volume are lower [12] (Fig. 20.2a).
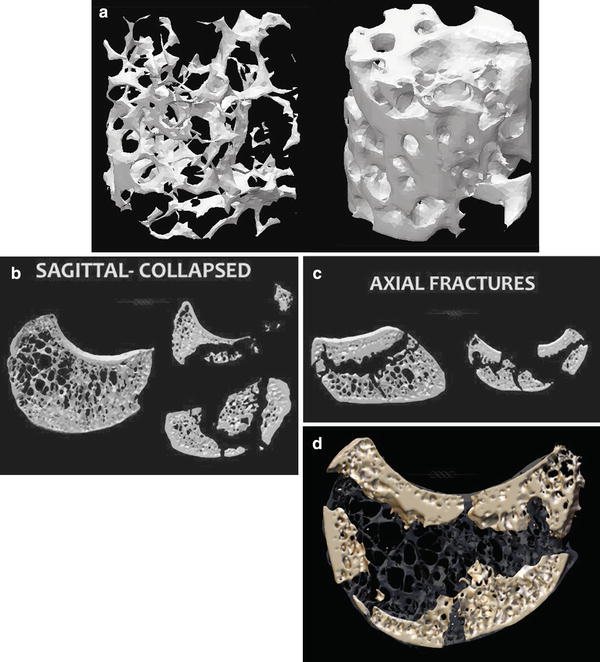
Fig. 20.2
(a) Micro CT scan of normal bone on the left, and bone from a lunate affected by Kienböck’s disease on the right. Note how the avascular, necrotic bone has larger, thicker trabeculae and is denser. (b) Sagittal micro CT images showing a normal lunate on the left and necrotic, collapsed lunates with multiple fractures on the right. (c) Sagittal micro CT images of avascular lunates with multiple fractures. The lunate on the left has a shear fracture in the axial plane. The fracture line has occurred at the junction between the hard bone of the subchondral bone plate and the weakened cancellous bone in the center. (d) Micro CT scan of the fragmented avascular lunate superimposed on a micro CT of a normal lunate. The bone of the hard subchondral bone plate is still present but there is loss of the longitudinal trabeculae, which leads to collapse and carpal shortening [Courtesy of Dr. Gregory Ian Bain]
It is the authors’ opinion that the subchondral bone plate is likely to be the critical part of the process of avascular necrosis, and that its survival is the key to the prognosis of articular cartilage, lunate, and the wrist. The normal lunate has longitudinal trabeculae that give axial support and prevent collapse of the bone during loading. As a result of the avascular necrosis, the trabeculae collapse and this leads to loss of height of the lunate and shortening of the carpus. In addition to the longitudinal collapse, shear fractures may occur with normal physiological loads, and with more advanced disease fractures occur through the proximal subchondral bone plate (Fig. 20.2b–d).
Late Chondral
The articular cartilage is often soft and can be indented, giving the impression that the articular surface has a false floor. The chondral changes will be described in more detail in the classification below.
Arthroscopic Classification
Bain and Begg first described their arthroscopic classification in 2006 [7]. This is based on the number of nonfunctional articular surfaces. The authors defined a normal articular surface as having a normal glistening appearance or minor fibrillation, with normal hard subchondral bone on probing. A nonfunctional articular surface is defined as having any one of the following: extensive fibrillation, fissuring, localized or extensive articular loss, a floating articular surface, or fracture. The number of nonfunctional articular surfaces determines the grade.
The authors observed a consistent pattern of changes in the lunate. This was based on MRI, plain radiographs and arthroscopy. The changes always first occurred on the proximal articular surface of the lunate. The more severe cases would develop a subchondral fracture and these would have secondary chondral changes in the lunate facet of the radius. Involvement of the distal articular surface of the lunate was rare, except if a coronal fracture extended through to the surface, or in late cases. The classification was based on these observations (Fig. 20.3).
Fig. 20.3
The Bain and Begg arthroscopic classification of Kienböck’s disease. The number of nonfunctional articular surfaces determines the grade. The grading system assists the surgeon to determine the best surgical option, based on the pathoanatomical findings. Although the classification was established based on arthroscopic findings, the grading can be determined based on imaging modalities [Reprinted from Bain GI, Durrant A. An articular-based approach to Kienböck avascular necrosis of the lunate. Tech Hand Up Extrem Surg. 2011;15(1):41–7. With permission Wolters Kluwer Health]
Grade 0
All articular surfaces are functional.
Grade 1
One nonfunctional articular surface—usually the proximal articular surface of the lunate.
Grade 2
Two nonfunctional articular surfaces. Divided into types A and B.
Grade 2A: The proximal lunate and the lunate facet of the radius.
Grade 2B: Proximal articular surface of the lunate, and distal articular surface of the lunate.
Grade 3
Three nonfunctional articular surfaces—the lunate facet of the radius, proximal and distal articular surfaces of the lunate, with a preserved head of capitate.
Grade 4
All four articular surfaces are nonfunctional.
The authors have noted the following observations [9]:
The degree of synovitis correlates with the degree of articular damage
The severity of articular changes are underestimated by plain radiographsRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








