Arthroereisis
Donald R. Green
Mitzi L. Williams
“Collapsing” pes planovalgus or flexible flatfoot is a complex pedal condition with numerous components. In its most significant form, it can lead to a disabling inability to ambulate efficiently. Various procedures are used to correct this deformity or to decrease the rate of progression. Arthroereisis is defined as “an operation for limiting motion in a joint in cases of undue mobility from paralysis, usually by means of a bone block” (1). The limitation of exogenous joint motion is without complete arthrodesis. Arthroereisis in the foot is a relatively modern surgical technique being used for collapsing pes planovalgus correction. In the foot, motion-blocking implants, placed within the sinus tarsi, have been designed to restrict excessive subtalar joint (STJ) pronation while preserving supination motion. Arthroereisis was originally designed for pediatric flexible flatfoot (2,3,4,5,6 and 7). However, many surgeons have expanded the indication for adults with or without posterior tibial tendon dysfunction (PTTD). It is also being used in certain rigid conditions if motion can first be restored (2,5,8,9,10,11,12,13 and 14).
HISTORY
Chambers was the first to develop the concept of arthroereisis for pathologic pronation of the foot (15). He noted that as the foot pronates, the talus plantarflexes and slides anteriorly until the lateral process of the talus contacts the floor of the sinus tarsi. (Actually, the lateral aspect of the talus rotates forward as the talus adducts and plantarflexes.) The talus is then blocked from further pronation. Chambers believed that by elevating the floor of the sinus tarsi, one could limit the plantarflexion and anterior excursion (adduction or internal rotation) of the talus and thereby prevent excessive pronation. To accomplish this goal, an autogenous bone graft from the tibia or the anterior calcaneus was placed under the leading edge of the posterior facet of the calcaneus to create a bony block for the lateral talus. This concept has served as the basis for many different arthroereisis procedures of the STJ.
Baker and Hill (16) performed an elevation of the posterior facet by inserting a lateral wedge of bone graft beneath the joint. This technique was purported to create a varus realignment of the posterior facet and thereby shift the remaining portion of the calcaneus beneath the talus. However, Vogler and Buckholz suggested that both these procedures result in subluxation of the remaining facets of the STJ (17,18).
LeLievre and Haraldsson employed autogenous bone grafts within the sinus tarsi to limit pronation. LeLievre used a free-floating bone graft obtained from the base of the proximal phalanx, which was resected as part of hallux valgus repair (19). Even though the graft was not fixed, LeLievre claimed that later surgical exploration in several patients revealed that the grafts were “alive, mobile, and painless.” Cartilage was said to have covered the osseous tissue. Haraldsson used bone graft within the sinus tarsi as well. However, he roughened the calcaneal surface to get bone attachment and then covered the dorsal surface with a soft tissue graft in an attempt to preserve the interface with the talus (20).
In 1977, Subotnick described arthroereisis with a free-floating sinus tarsi Silastic implant (21,22). Since then, various surgeons have designed implants specifically for the sinus tarsi area. Smith designed the disk and peg (STA-peg—Wright Medical) (23,24) (Fig. 48.1); Valenti, the threaded polyethylene cylinder (Fig. 48.2); and Viladot, the Silastic champagne glass implants, respectively (Fig. 48.3). Other implants were introduced by Addante (Silastic sphere) (8,25), Sgarlatto (Silastic mushroom) (Fig. 48.4), and Pisani (the stainless steel screw with the Silastic crown). Lundeen modified the STA-peg by applying an inclined platform (LSI-Sgarlatto Labs) (26) (Fig. 48.5). Flake and Austin altered the technique of the disk and peg insertion (9,27,28) (Fig. 48.6), while Maxwell and Brancheau’s popular threaded cylinder (MBA) (Fig. 48.7), Giannini’s expanding cylinder with screw, Graham’s HyProCure (Gramedica, Shelby Township, MI), and Villadot’s Kalix continue to be studied. Modifications of these implants have been made more recently. Sgarlatto Labs (LSI) and Tornier Labs (formerly Futura-ASI) have modified the disk and peg implants by softening the edges and lengthening the stems (Fig. 48.8). Tornier Labs added regular and extra-thick disk sizes. Tornier has modified both the mushroom dome implant with polyethylene material (ADI) and the threaded cylinder-type implant (ACI), as have many others.
CLASSIFICATION
To date, these implants are categorized into one of three groups. Based upon an implant’s biomechanical properties, Vogler classified the implants as a self-locking wedge, an axisaltering prosthesis, or an impact-blocking device (17,18). A self-locking wedge can be any material inserted or implanted into the lateral sinus tarsi, which restricts eversion of the STJ. The implant prevents contact of the lateral talar process with the floor of the sinus tarsi, otherwise restricting pronation. The MBA (Kinetikos Medical Inc., Carlsbad, CA), for example, supports the talar neck while limiting plantarflexion and adduction of the talus during end range of pronation (5,12). The titanium implant is hollow and allows for soft tissue growth. There are many other axis-altering devices that fit into this category. Many have modified shapes, and some relatively new ones are even bioabsorbable. Classically, the LeLievre bone graft and Subotnick Silastic plug procedures are self-locking wedge types.
The second group is referred to as axis-altering devices. These implants actually elevate the STJ axis and therefore reduce calcaneal eversion. The disk and peg implants can be used in this manner when the stem is placed traditionally in a vertical orientation in the floor of the calcaneus as described by Smith and Millar (23,24). The disk elevates the floor of the sinus tarsi, altering the STJ axis. The leading edge of the posterior
facet of the talus rides up on the disk to prevent excessive plantarflexion of the talus. This limits the excessive STJ pronation. Unfortunately, this does not work as well with a high STJ axis (transverse planar dominant STJ).
facet of the talus rides up on the disk to prevent excessive plantarflexion of the talus. This limits the excessive STJ pronation. Unfortunately, this does not work as well with a high STJ axis (transverse planar dominant STJ).
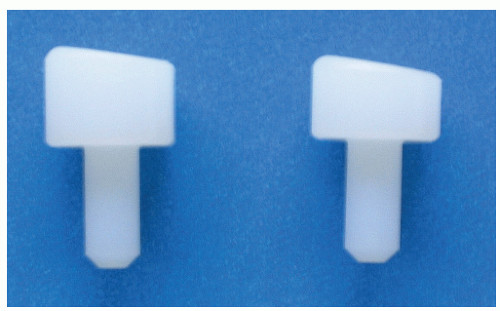 Figure 48.1 The angled subtalar arthroereisis-peg device. The stem is inserted into the floor of the sinus tarsi while the angled implant resists anterior displacement of the lateral talar process. |
The final group is referred to as impact-blocking devices or direct-impact implants. Without changing the STJ axis, these implants limit anterior displacement (adduction) of the lateral talar process. Examples are the Sgarlatto mushroom, the Tornier ADI, and the Flake-Austin disk and peg technique using the ASI, LSI, or STA-peg implants (9,27,28) (see Fig. 48.6). These all block the lateral process of the talus from advancing beyond the posterior facet of the calcaneus.
Overall, arthroereisis via any type of implant has been developed to restrict excessive pronation of the STJ in all ages and to bypass adaptive changes in children (17,18,29,30 and 31). With such a vast array of implants and numerous surgical techniques described, the specific implant chosen is often based on the surgeon’s personal experience. This concept makes it essential to evaluate the biomechanics of the STJ and radiographic findings both before and after arthroereisis.
BIOMECHANICS
The STJ is a triplanar joint whose axis varies in spatial location throughout its range of motion. The axis generally courses posterior, plantar, lateral to anterior, dorsal, and medial. The average STJ maintains equal amounts of transverse and frontal plane motion although there is a wide individual variance (32). The ankle joint generally takes care of the majority of the sagittal plane motion in the rearfoot. Root et al (32) stated the average STJ range of motion to be 30 degrees in which 20 degrees of inversion and 10 degrees of eversion were available from what they described as the “neutral” position. Excessive pronation is available in the flexible pes planovalgus foot and is apparent throughout gait. Closed kinetic chain pronation can be visualized as calcaneal eversion and/or talar tibial inversion, talar plantarflexion, and adduction. It is the excessive closed kinetic chain pronation that arthroereisis is meant to restrict. By resetting the maximally pronated position of the STJ, there is less calcaneal eversion and foot abduction. The arthroereisis reduces pathologic pronation and is able to stabilize the foot for proper propulsion. Husain and Fallat (11) who found forefoot changes with improved first ray stability also supported these results and radiographic changes. When executed correctly, arthroereisis may reduce detrimental forces in the adult patient following soft tissue repair for stage II adult acquired flatfoot and bypass adaptive changes that occur among children (18,30,31,33).
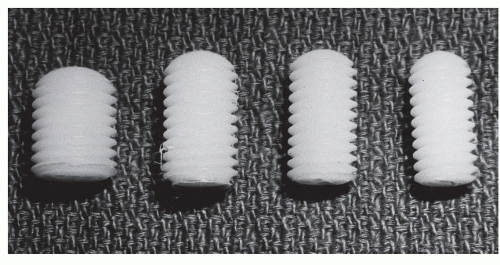 Figure 48.2 The Valenti device. This threaded implant was inserted into the sinus tarsi and was screwed into position with specific instruments designed for this procedure. |
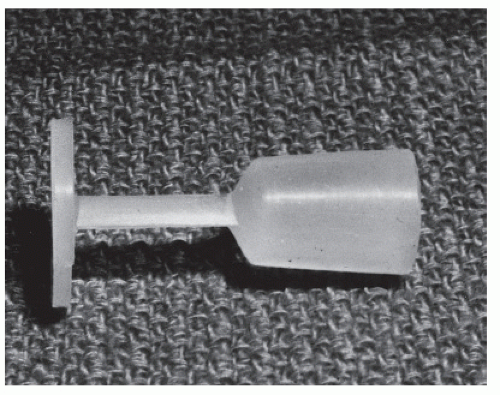 Figure 48.3 The Viladot device. The implant was inserted into the sinus tarsi with the stem and “umbrella” passed medially and pulled out the canalis tarsi just posterior to the sustentaculum tali. This was designed to prevent lateral extrusion of the implant, a problem previously encountered with earlier Silastic plugs. |
Similar to other surgical flatfoot correction, a mildly everted heel in the maximally pronated stance position is the proper positioning of the rearfoot (9,11,12,27,28,34,35). Since some pronation is necessary for normal gait, it is essential not to overcorrect the foot when performing subtalar
arthroereisis procedures. The calcaneus should be allowed to evert 2 to 4 degrees beyond the perpendicular in its maximally pronated position for normal function. Arthroereisis implants come with different sizers for proper positioning. However, overcorrections do occur that result in a varus rearfoot and will lead to postural symptoms, lateral forefoot pressure, and fatigue (2,9,28).
arthroereisis procedures. The calcaneus should be allowed to evert 2 to 4 degrees beyond the perpendicular in its maximally pronated position for normal function. Arthroereisis implants come with different sizers for proper positioning. However, overcorrections do occur that result in a varus rearfoot and will lead to postural symptoms, lateral forefoot pressure, and fatigue (2,9,28).
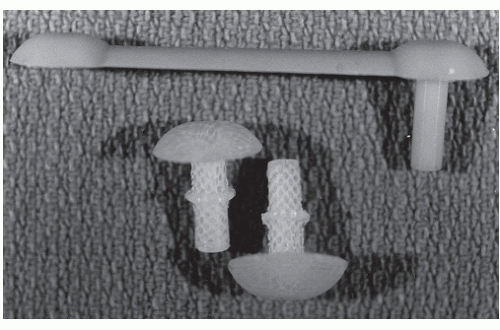 Figure 48.4 The Sgarlatto device. This was inserted into the floor of the sinus tarsi. Forward motion of the lateral process of the talus was blocked by the implant. |
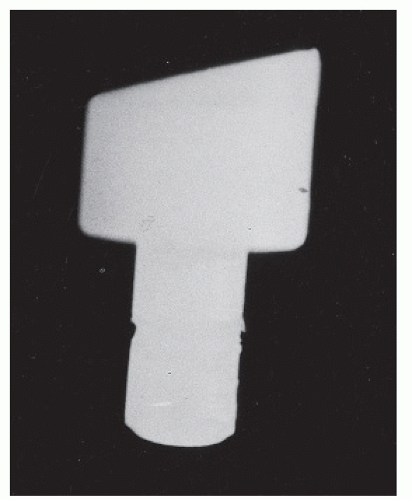 Figure 48.5 The “inclined” subtalar arthroereisis-peg device. The thicker portion is placed anteriorly to resist the anterior displacement of the lateral process further. |
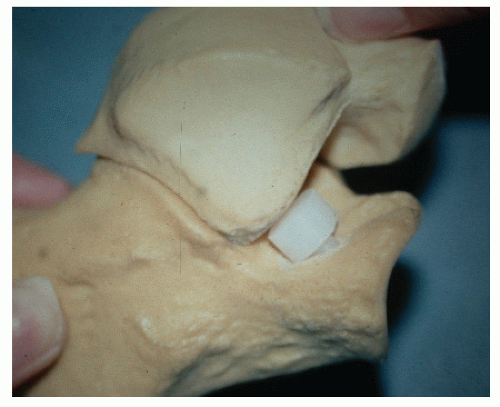 Figure 48.6 The subtalar arthroereisis-peg device. The lateral process of the talus rests on the superior surface of the platform. The implant serves as an axis-altering device. |
 Figure 48.7 The Maxwell-Brancheau arthroereisis device. This threaded device is inserted into the sinus tarsi. |
The “neutral” STJ position, according to Root, is when the STJ is congruous (32). The talonavicular joint is noted to be smooth medially with no bulge of the talus or the navicular. The area of the sinus tarsi is neither stretched nor taut. In a neutral stance position, the calcaneus is often slightly inverted to the ground. With significant tibial varum or more proximal frontal plane deformity, the neutral stance inversion can be quite significant. Both the neutral subtalar position and the maximally pronated position of the STJ can be reproduced intraoperatively. However, the calcaneal position relative to the ground cannot be determined intraoperatively. Therefore, it is essential preoperatively to determine how far the desired calcaneal position (2 to 4 degrees everted from the perpendicular) is from
the neutral position and/or the maximally pronated position in stance (Fig. 48.9). This allows appropriate calcaneal eversion in gait, allows adequate pronation for shock absorption, and prevents overcorrection (9,28). The desired maximally pronated postoperative stance position can accurately be estimated intraoperatively between the maximally pronated and neutral subtalar positions.
the neutral position and/or the maximally pronated position in stance (Fig. 48.9). This allows appropriate calcaneal eversion in gait, allows adequate pronation for shock absorption, and prevents overcorrection (9,28). The desired maximally pronated postoperative stance position can accurately be estimated intraoperatively between the maximally pronated and neutral subtalar positions.
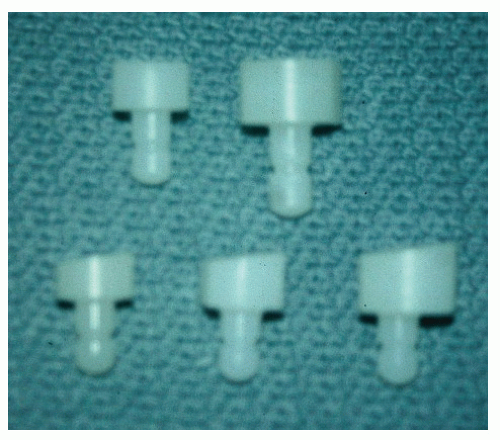 Figure 48.8 The subtalar arthroereisis-peg device. Implant is available in various sizes and the angled design. |
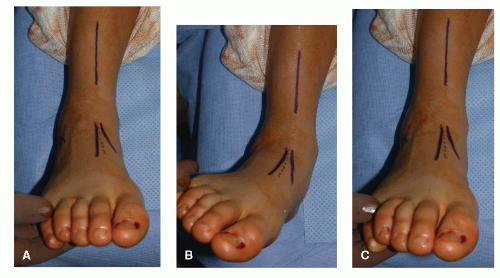 Figure 48.9 A: Neutral position. B: Maximally pronated position. C: The dotted line indicates goal for postoperative pronation. |
Arthroereisis has produced varying results according to different designs, authors, and surgeons. The majority of clinical and radiographic analyses demonstrate that the procedure is successful. Still, it was not until 1996 that the precise biomechanical influence of arthroereisis had been researched and documented. Christensen et al (36) investigated 11 fresh frozen cadaver specimens using a three-dimensional radio wave tracking system. Tarsal bones were monitored with and without implantation of an ultrahigh-molecular-weight polyethylene peg and disk implant (angulated at 8 degrees). Closed kinetic chain motion was simulated by axially loading the specimens to 756 N (one bodyweight). Ultimately, the talus externally rotated and dorsiflexed and the navicular inverted and slightly dorsiflexed, while the cuboid and calcaneus both inverted from the maximally pronated position. The navicular also proved to invert relative to the cuboid. These results confirmed supinatory effects (or reduced pronatory effects) of STJ arthroereisis by using fresh frozen specimens. In addition to a significant stabilizing effect at the STJ, the implant controlled motion throughout the entire rearfoot complex through joint coupling. In essence, the technique exerts a physiologic supinatory influence on the tarsus during weight-bearing, with resultant motions occurring along the same directional parameters as in normal joints. Furthermore, the implant does not appear to block the independent movements across the STJ. A restriction of excessive pronation could only assist in relief of symptoms and decrease the rate of progression of the deformity much like an external orthosis.
INDICATIONS
Subtalar joint arthroereisis is indicated when conservative treatment is inadequate to control pathologic STJ pronation in flexible pes planovalgus deformity. The procedure has generally been employed in patients who have not yet reached skeletal maturity. However, these devices have been used with success in older patients and in some instances may be a reasonable alternative to arthrodesis procedures (34,37,38).
Although some degree of pain is frequently present with pes planovalgus deformity, the absence of pain does not preclude surgical intervention. The full functional demands the foot is expected to tolerate are frequently absent in the younger patient who does not participate in athletic activities. Children frequently fail to communicate minor pain and discomfort. Questioning of the parents often reveals the subjective complaints of clumsiness, postural fatigue, and refusal to walk long distances or participate in activities. Aching pains in the legs or feet, excessive medial shoe wear or posterolateral heel wear, or medial foot cramps or soreness can oftentimes be elicited from the parents. These subtle alterations in normal behavior provide useful clues to assessing the degree of disability arising from the pathologic pes valgus deformity. These signs should be considered abnormal in a growing child and should not be explained or discounted on the basis of growing pains (9,28).
In 2003, Viladot et al (39) evaluated the Kalix in STJ arthroereisis in the sinus tarsi for stage II PTTD. He concluded that a flexible flatfoot, attributed to posterior tibial tendon pathology, requires correction of bone position and proper talar positioning. Contrary to this, he believed that trying to normalize the talus position via arthroereisis in an uncorrected flatfoot from childhood would lead to ankle arthrosis. In the moderately long-term results, this has not proven to be the case with the arthroereisis procedures in general (9,20,28).
Likewise in 2003, Myerson et al concluded out of 43 MBA prostheses (31 children and 12 adults) that 60% of these feet required additional correction such as an Achilles lengthening or gastrocnemius recession. His indications among children were a flexible flatfoot with or without association of an accessory navicular or tarsal coalition. For adults, indications were flexible flatfoot with or without posterior tibial tendon rupture or sinus tarsi pain. Further, he explained the procedure due to its minimal invasiveness may benefit the elderly with sinus tarsi pain associated with flexible flatfoot deformity. He avoided resecting the interosseous ligament and determined patients with a large degree of talonavicular uncovering after
a calcaneal medial displacement osteotomy benefited from arthroereisis.
a calcaneal medial displacement osteotomy benefited from arthroereisis.
A total of 40 disk and peg procedures were evaluated subjectively and objectively by Forg et al (9) in 2001, with an average age group of 9.7 years. In 2003, Dickerson et al (28) reported on 87 disk and peg procedures involving 44 patients with an average age of 9 years and follow-up of 6.5 years. The authors applied the Flake-Austin modification in both cases, which involved placing the peg into the calcaneus at approximately a 45-degree angle so that the dorsal disk came into complete contact with the lateral leading wall of the talus. The indication was pediatric flexible flatfoot. Clinical signs and symptoms included night cramps, pain with walking and standing, fallen arches, lower back and/or knee pain, resistance to prolonged walking, inability or lack of desire to participate in sports, abnormal shoe wear, decreased coordination, and arch pain. All groups of signs and symptoms were significantly reduced except night cramps in the Forg study. Many of these children had become much more active in weight-bearing activities and sports, and it was postulated that this played a significant role in the increase. No patients were worse off. Ninety-five percent of the patients in both studies would recommend or highly recommend the procedures.
The indications for arthroereisis are still being refined. Research supports its use in flexible pediatric collapsing pes planovalgus deformity. Timing of the procedure remains important in pediatrics. When used in younger children, especially those that are not mature enough for osseous procedures such as the Evans and Cotton osteotomies, arthroereisis can decrease the progression of deformity. As for its implication in adult PTTD, uses continue to be explored. Arthroereisis may function in an adjunctive manner to a soft tissue procedure or as a second point of fixation combined with arthrodesis.
CLINICAL EVALUATION
One clinical feature of many patients with flexible pes valgus deformity is a foot that appears essentially normal during non-weight-bearing but pronated when the patient is standing. Severe depression and obliteration of the medial arch are frequently present, as the talus and midfoot adduct and plantarflex. These findings may not be as obvious or may be absent in the pronated cavus foot. Severe pronation of the STJ may occur without complete obliteration of the medial longitudinal arch, and this feature should not preclude surgical correction.
The plane of deformity and the ability of the midtarsal joint to resist deforming sagittal plane forces or unlocking are essential in assessing the usefulness of arthroereisis. Failure of the midtarsal joint to be able to adequately resist dorsiflexion of the forefoot on the rearfoot will result in increased flattening of the medial and lateral longitudinal arches. This is typically found in association with transverse plane deformities. Patients with little to no change in midtarsal joint pronation or stability, with varying changes in STJ position, are likely poor candidates for the procedure alone. An Evans calcaneal lengthening osteotomy may be required.
Arthroereisis is also ineffective when there is a true structural calcaneal valgus (not just an everted calcaneus) that is nonreducible. Caution must also be exercised when there is a high degree of rear foot varus, especially if this is only partially compensated.
Both clinical and radiographic assessment allow for determining the plane of deformity (9,28,40,41). The plane of deformity can assist with procedure selection. An axis-altering device is primarily used in frontal plane disorders (Fig. 48.10). With STJ pronation, the front edge of the implant moves over the implant. This new axis created per the implant is oriented more vertically. An example of such an implant is the classic vertical placement of stem of the disk and peg implant a la Smith and Millar (24).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


