Salvage Arthrodesis for Charcot Arthropathy
Keywords
• Arthrodesis • Charcot • Limb salvage • External fixation • Ulceration
Epidemiology
Charcot osteoarthropathy, also known as neuropathic osteoarthropathy, is a syndrome that results in the destruction of single or multiple joints leading to permanent joint deformity.1 Joint changes as a result of neuropathic change were first described by Musgrave in 1703.1 Most commonly credited with modern day definition of this condition is Jean Marie Charcot2 for his 1868 analysis of neuropathic osteoarthropathy in patients with tabes dorsalis.
Currently, Charcot osteoarthropathy is most commonly associated with diabetes mellitus as the primary origin, but has been attributed to multiple conditions. Charcot osteoarthropathy has also been reported in connection with infection, spinal or peripheral nerve injury, alcoholism, trauma, cerebral palsy, syphilis, spina bifida, and multiple other medical disorders.2 The identifying characteristic commonly shared among these conditions is significant decrease or loss of pain sensation to the area in question. In addition to neuropathy, previous authors suggest the presence of several other factors that may play contributing roles in the Charcot foot, including trauma, metabolic factors, arteriovenous shunting abnormalities, and absence of occlusive arterial disease.3
Historically, this condition is reported to affect a very small population, namely only 0.2% of the diabetic population, with a higher incidence reported among the diabetic population previously diagnosed with peripheral neuropathy.2 Studies suggest that a significant number of Charcot cases go undiagnosed because of lack of clinical recognition by physicians, leading to more severe deformity in this patient population.4,5 Early and accurate diagnosis of acute Charcot osteoarthropathy is of extreme importance in the clinical management of this condition.5
Diagnosis/imaging
Diagnosing acute Charcot can be difficult. Patients typically present with significant localized edema, erythema, and warmth in the affected limb compared with the contralateral limb. Because of the common trio of symptoms on presentation, patients are often misdiagnosed with cellulitis, gout, or deep venous thrombosis.6 Misdiagnosis of Charcot can lead to patients following incorrect treatment protocol, including antibiotic therapy; the absence of an offloading program, resulting in increased deforming forces on the limb; and even unnecessary amputations. An increased suspicion for Charcot is essential among the neuropathic diabetic population presenting with the aforementioned symptoms. Pedal pulses are typically present in patients with Charcot foot, because concomitant peripheral arterial disease is uncommon.6 Patients with advanced Charcot or a previous history of the condition may present with an already deformed foot type. These patients commonly present with a rocker-bottom foot and are often affected by ulcerations plantarly.
Charcot osteoarthropathy primarily should be diagnosed clinically, but then plain film radiographs are useful in staging the condition and following its progression. The Charcot foot was originally classified radiographically by Eichenholtz7 in 1966, who described three distinct developmental stages. Stage 1 is described as subchondral fragmentation and referred to as the development stage. Stage 2 is known as the coalescence stage, with absorption of small debris and fusing of larger fragments of bone, with notable sclerosis at both the proximal and distal aspect of the previously fragmented bone. Stage 3 is referred to as the reconstructive phase, with remodeling of the previously fragmented and recoalesced bone. Yu and Hudson8 added a stage 0 to the Eichenholtz system for patients with diabetes, adding clinical signs of inflammation and trauma to the foot before radiographic evidence of the condition is noted.
A five-stage classification system was proposed by Sella and Baratte9 in 1999. Stage 0 was defined as a clinical diagnosis with lack of radiographic evidence. Stage 1 included clinical findings and localized osteopenia, diastases, and cyst formation visualized on plain film radiograph. Stage 2 was defined as involving the presence of joint subluxation. Stage 3 involved significant collapse of the medial arch of the foot. Stage 4 was described as radiographic evidence of boney fusion with notable sclerosis in the areas of previously fragmented bone. An additional classification system that identifies specific joint involvement was described by Sanders and Frykberg,10 which is helpful in identifying a specific location of involvement in the foot.9
Multiple imaging studies can be used in conjunction with or in addition to plain film radiograph. Triphasic bone scan has been historically used as a tool in identifying Charcot osteoarthropathy, although its usefulness is currently debated, because it is a nonspecific study and does not differentiate between Charcot osteoarthropathy and osteomyelitis.11 More recently, use of a white blood cell–labeled bone scan has been proposed because of its ability to exclude osteomyelitis as a differential diagnosis, and is considered by many as the gold standard for differentiation.11 MRI is also used by many physicians to differentiate Charcot from osteomyelitis, although widespread debate exists as to its ability to do so. Despite the fact that it is a poor tool for differentiation, some describe it as the gold standard for evaluating extent of involvement of either process.11 The use of imaging studies to correlate a clinical diagnosis of Charcot osteoarthropathy and to evaluate progression of the condition can prove useful when assessing a treatment protocol for a patient.
Medical treatment
The widely accepted initial treatment protocol after diagnosis of acute Charcot osteoarthropathy is complete offloading of the extremity with total contact casting, and local wound care for any ulceration.12 Offloading the affected extremity avoids any deforming weight-bearing forces placed on the foot. The recommendation is for patients to remain non–weight-bearing in a total contact cast until all clinical and radiographic evidence of acute Charcot osteoarthropathy has dissipated, with the average length of casting reported as between 3 and 4.5 months.13
Pharmacologic intervention in the treatment of Charcot osteoarthropathy has recently been proposed to inhibit osteoclastic activation and excessive inflammatory response.12 Bisphosphonates used in antiresorptive therapy have been shown in randomized trials to have a positive effect in patients with acute Charcot, helping to decrease foot temperature, with a decrease in bone turnover markers and no notable side effects.14 The use of pharmacologic modalities as an adjunct to offloading therapy in the treatment of the Charcot foot is promising but currently lacking long-term large-scale studies to prove its efficacy.
Midfoot arthrodesis
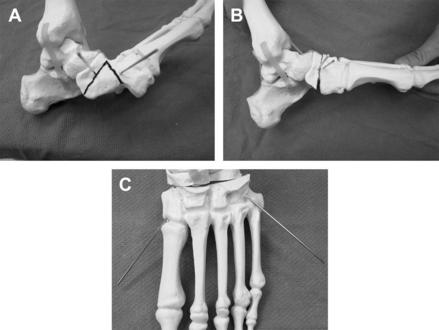
The authors have noticed that when they follow these indications for salvage arthrodesis, the success of limb salvage increases through decreasing the rate of ulcer formation. The operative goal of any surgical procedure is to establish a stable plantigrade foot that can be fitted in a custom molded shoe or device, and to prevent ulceration. Contraindications to performing this procedure are the presence of bone infection, poor vascular supply, known poor patient compliance, poor nutritional status, or elevated or abnormal laboratory values that indicate poor wound healing. When treated with simple ostectomy, midfoot ulcers beneath the lateral column have a higher incidence of reulceration than those beneath the medial column. Therefore, lateral midfoot ulcers associated with Charcot deformity should be treated with arthrodesis.15 Hamilton and Ford16 stated that if bony resection of a midfoot prominence leaves an unstable structure, then progression of the rocker-bottom deformity and recurrent ulceration are likely. This article’s authors strongly discourage and rarely perform simple ostectomies of the midfoot. They believe in correcting the deformity to prevent any future recurrences, and routinely perform a midfoot wedge osteotomy (Fig. 1). This osteotomy can correct deformities in the transverse and sagittal plane.
Some controversy exists in the literature regarding the appropriate timing of surgery. Some authors advocate performing the fusion procedure while in the acute stage, whereas others prefer waiting until the later stages of the Charcot process. Simon and colleagues17 evaluated the use of arthrodesis of the tarsometatarsal area for the treatment of Eichenholtz stage 1 Charcot arthropathy. All 14 arthrodesis procedures were successful, resulting in anatomic alignment and clinical union. No patients had immediate or long-term complications, and none reported ulceration after the operation. Before this study, it was accepted that all fusions in a Charcot foot should wait until Eichenholtz stage 2 or 3 because performing the procedure earlier would lead to poor outcomes and further fragmentation and bony destruction. This study showed that fusing in stage 1 is easier because no gross deformity is present and excessive bony work is not necessary. The authors postulated that operating in the early stage did not seem to lengthen healing time and in fact may have expedited the reversal of the destructive process.
In another study, Roukis and colleagues18 treated eight unstable Eichenholtz stage 1 diabetic Charcot foot deformities using open reduction internal fixation, immobilization in a non–weight-bearing cast for 8 to 10 weeks, and then a total-contact weight-bearing cast for 2 to 7 months. These feet remain stable and free from ulceration at a mean of 28 months.18
Studies have supported performing arthrodesis in Eichenholtz stage 2 and 3 Charcot feet with good results. Papa and colleagues18,19 reviewed 29 patients who had osseous prominences with instability, performed an arthrodesis with open reduction internal fixation, then cast immobilization and finally custom ankle foot orthoses were used. At a mean of 5 months, 19 patients (66%) developed a solid arthrodesis, 10 patients developed a pseudoarthrosis, and 7 were stable. None of the patients treated who developed a solid arthrodesis or stable pseudoarthrosis broke down during the follow-up period of 43 months.
Early and Hansen20 reviewed 21 feet with Eichenholtz stage 2 and 3 diabetic Charcot foot and osseous deformities with instability. They performed arthrodesis with open reduction internal fixation, tendo-achilles lengthening, cast immobilization, and wheelchair use. At a mean of 28 months, 18 feet (86%) had been treated successfully.
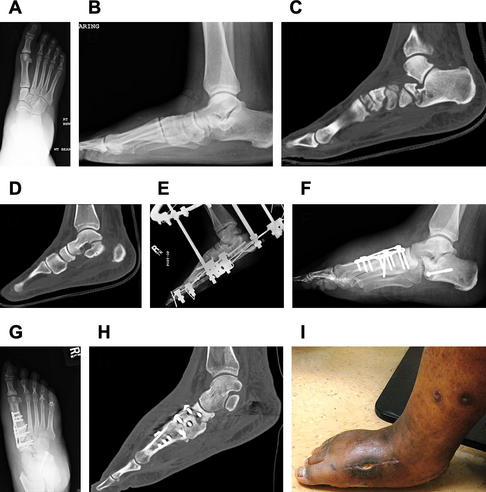
The authors have performed arthrodesis of the medial column and the entire midfoot complex with open reduction internal fixation in both the early and late stages of the Charcot process. They prefer to wait and use open reduction internal fixation in the late stages in additional to external fixation, and solely use external fixation in the early stages of the process. They believe it is difficult to perform an open reduction internal fixation in the acute Charcot process because of edema, obliteration of the soft tissue planes, and the soft fragmented bone. One can easily gouge excessive bone while resecting cartilage and debris from the joint surfaces because of lack of strength of the bony structures. Apposition of bony surfaces could potentially become more difficult. The authors treated an acute Charcot midfoot (Fig. 2) initially with external fixation, and soon after the patient experienced what is known as “cage rage” and the external fixator was removed. After removal, a medial column fusion was performed with a “superconstruct” plate, specifically designed for Charcot reconstructions. The patient progressed to a solid fusion, which is evident on postoperative advanced imaging, without complications. She is now ambulating in custom molded ankle foot orthoses and diabetic shoes. In this one case, the authors were able to achieve a solid fusion of an acute Charcot foot and prevent further progression of deformity.
The authors have used various techniques to achieve midfoot fusion in a Charcot foot. Fusion can be accomplished through internal fixation, external fixation, or a combination of both. They usually advocate a combination of internal and external fixation devices to achieve an adequate fusion of the Charcot foot (Fig. 3). A recent technique described in the literature is beaming for midfoot arthrodesis. Beaming uses axial intramedullary large-diameter screws to realign the medial and lateral columns. Rooney and colleagues21 introduced a technique of axial intramedullary fixation of the medial and lateral columns using long intramedullary screws. Assal and Stern22 used a medial column intramedullary screw in 15 patients with Charcot with rocker-bottom deformity, 13 of whom had a plantar ulceration. All the patients underwent realignment with arthrodesis. At a mean of 42 months’ follow-up, 14 patients were able to walk and no recurrent ulcers were seen. The investigators stated that a key advantage to using axial intramedullary fixation is that much less dissection is required to insert the screw than to place a plate. They state that this technique prevents vascular compromise to the bone and decreases the rate of wound complications.

Related posts:
 and Considerations of Foot and Ankle Arthrodesis
Soft Tissue Closure of Severe Diabetic Foot Infections: A Combination of Biologics, Negative Pressure Wound Therapy, and Skin Grafting
Joint Arthrodesis
Metatarsophalangeal Joint Arthrodiastasis and Biologic Resurfacing with External Fixation: A Case Report
Arthrodesis
Arthrodesis
and Considerations of Foot and Ankle Arthrodesis
Soft Tissue Closure of Severe Diabetic Foot Infections: A Combination of Biologics, Negative Pressure Wound Therapy, and Skin Grafting
Joint Arthrodesis
Metatarsophalangeal Joint Arthrodiastasis and Biologic Resurfacing with External Fixation: A Case Report
Arthrodesis
Arthrodesis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


