Fig. 3.1
Route of the Hueter approach
In this chapter, we present the surgical technique and our results and discuss the advantages and disadvantages of the concept.
Surgical Technique
General anaesthesia is preferable in athletic patients to achieve optimal myorelaxation.
The level of neuromuscular blockade following curarisation is checked prior to the femoral phase, and there is close collaboration with the anaesthetists.
Installation
The patient is placed in lateral decubitus on a conventional operating table with the posterior distal section removed.
The pelvis is stabilised for an anterior approach with support to the sacrum and pubis; the hip is flexed at 15°.
The lower extremity rests on two supports, one supracondylar and the other under the distal fourth of the leg. The posterior space enables luxation of the limb with complete freedom of movement using its weight alone in external rotation, extension, and adduction (Fig. 3.2).

Fig. 3.2
Patient installation in lateral decubitus on a conventional table
A sterile bag is placed behind during the femoral phase, protecting the leg held vertically.
Incision
The oblique incision, 8–10 cm in length, is made over the neck of the femur along a line running from the anterior-superior iliac spine two fingerbreadths from the summit of the greater trochanter (Fig. 3.3).

Fig. 3.3
Oblique incision from the anterior-superior iliac spine to summit of the greater trochanter
Intermuscular Approach
The tensor fasciae lata is exposed (TFL): its aponeurosis is incised using a scalpel blade following the direction of the fascial fibres, 5 mm below (Fig. 3.4). The anterior edge of the muscle body is freed using Mayo scissors and then blunt finger dissection. Once the muscle has been bypassed, we have direct access to the anterior cervical region.
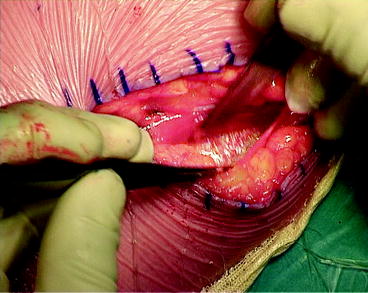
Fig. 3.4
Incision of the aponeurosis of the tensor fasciae lata
A modified Charnley frame is placed against the body of the TFL laterally and on the sartorius medially. One cobra retractor is placed at the superior base of the neck under the gluteus minimus and a second retractor to retract the distal body of the TFL out of the surgical field.
The superficial aponeurosis of the rectus femoris is incised and the muscle body retracted inwards. The deep aponeurosis is then carefully incised and the anterior circumflex pedicle dissected and ligated. The tubercle for the insertion of the vastus lateralis muscle can be seen under its lateral stump; this is an essential landmark for the arthrotomy. Using a periosteal elevator, the capsule is then lifted along a line from the insertion of the rectus femoris to the tubercle of the vastus lateralis, with the limb held in slight rotation and flexion without constraint.
Arthrotomy
The arthrotomy is performed at the superior edge of the neck, from the insertion of the rectus femoris to the tubercle of the vastus lateralis (Fig. 3.5). An initial debridement is performed at the base of the neck towards the lesser trochanter along the inter-trochanteric line to free the large anterior capsular flap, which is preserved. A second debridement is then performed at the base of the neck towards the trochanteric fossa respecting the insertion of the gluteus minimus.
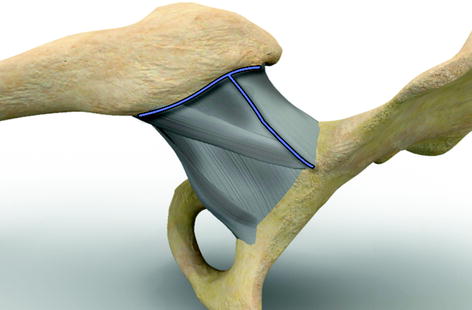
Fig. 3.5
Incision of the anterior capsule
The cobra is then put back between the rim and the apical capsule; a Hohmann retractor is placed between the anterior capsule and the rim. The head of the femur is broadly exposed; the rim is resected using a scalpel blade.
Cervicotomy
A retractor is placed under the neck, with the lower limb slightly flexed with external rotation to expose its anterior aspect as much as possible.
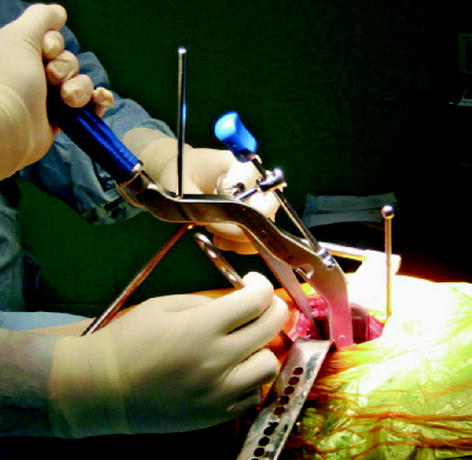
The preoperative landmarks of the length of the lower extremity are transposed from the vertical axis to the tubercle of the vastus lateralis. The vertical impaction of a straight chisel, from the base of the neck to the tubercle, enables an appropriate initial, yet incomplete, vertical cervicotomy without the risk of posterior bleeding. Motorised section is then performed using a narrow rigid blade, along the plane of the superior edge of the first prepositioned reamer (Fig. 3.6).
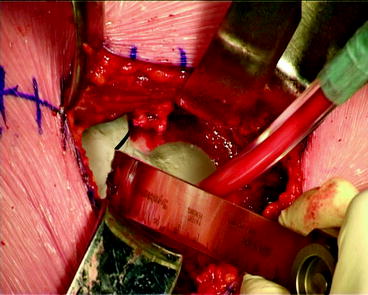
Fig. 3.6
Cervicotomy with the oscillating saw
Impaction of the straight chisel in the cervicotomy site enables exposure of the cervical section via deflexion. A Lambotte lag screw is screwed in the centre of the head subchondrally; the neck is twisted through 3–4 rotations to avulse the round ligament. The posterior synovial fringes are cut using a scalpel blade. The head is then removed and calibrated.
Acetabular Preparation
The lower extremity is repositioned on its supports.
A Steinmann pin is impacted vertically from the roof of the acetabulum pushing back the anterior edge of the proximal muscle mass of the TFL. The Charnley frame is repositioned horizontally to rest on the distal body of the muscle. The acetabulum is then exposed using two Hohmann retractors resting on the anterior and posterior horns.
The table is lowered.
The residual rim and round ligament are resected, and the transverse ligament is preserved.
Haemostasis of the obturator is systematic.
Instrumentation of the acetabulum is performed vertically, with reaming at 45° (Fig. 3.7).
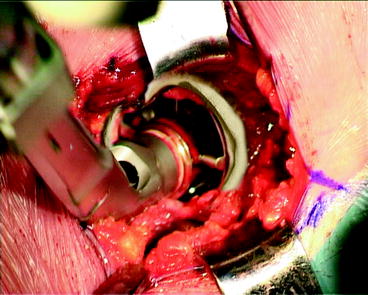
Fig. 3.7
The acetabulum is prepared with reamer
The handle is also angled at 45° and ensures polar pressurisation but with the mediation of the transverse acetabular ligament, thus reproducing the patient’s normal anteversion (Fig. 3.8). The exposed subchondral bone must be preserved. The press fit is tested with a trial cup.
 Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
The Anterolateral Watson Jones Approach in Total Hip Replacement in the Supine Position
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
The Anterolateral Watson Jones Approach in Total Hip Replacement in the Supine Position
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing




Related posts:
Smith-Petersen Approach and Lateral Position with Mini-Stem
Mini-Invasive Approach and Navigation in Total Prosthesis of the Hip
The Anterolateral Watson Jones Approach in Total Hip Replacement in the Supine Position
Anterior Approach for Total Hip Arthroplasty: Technique Without Fracture Table
Minimally Invasive Posterior Approach: Technical Evaluation, Initial Results and Follow-Up at Two Years
Navigation and the Square Angle Pointer in Hip Resurfacing
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
