Anterior Ankle Arthroscopy: Indications and Surgical Techniques
Gregory C. Berlet
INTRODUCTION
Arthroscopy of ankle allows the direct visualization of intra-articular structures without an arthrotomy or osteotomy. Advances in technology with improved video, small joint instrumentation, and noninvasive distraction, combined with the demand for minimally invasive treatment have expanded indications for arthroscopic-mediated care of the ankle. Over the past decade, these advances have forwarded anterior ankle arthroscopy as a necessary skill for the orthopaedic surgeon.
ANKLE ARTHROSCOPY—OVERVIEW
Anterior ankle arthroscopy is a well-established procedure used for both accurate diagnosis and operative management of many ankle disorders. Arthroscopic surgery of the anterior ankle allows the direct visualization and manipulation of intra-articular structures including bone, cartilage, and ligamentous structures.
Diagnostic indications for the use of ankle arthroscopy include unexplained pain, swelling, stiffness, instability, hemarthrosis, and locking or popping, as well as a negative workup in a patient with symptoms unresponsive to a thorough conservative treatment program.
Therapeutic indications include injuries of the articular cartilage and soft tissue, bony impingement, débridement of soft tissue lesions, synovectomy and loose body removal, arthrofibrosis, ankle fractures, and osteochondral defects. Ankle arthroscopy can also be used in ankle stabilization procedures and arthrodesis, as well as for irrigation and débridement of septic arthritis.
ANATOMY RELEVANT TO ANTERIOR ARTHROSCOPY
The congruency of the distal tibia and talar dome makes arthroscopic visualization difficult through a single portal. The distal tibia is concave in the sagittal plane and convex in the coronal plane. The anterior tibial plafond is slightly convex with a medial notch (notch of Harty), which recedes approximately 4 mm, near the junction of the plafond with the medial malleolus. This is an ideal location for introduction of the arthroscopic instruments. The medial malleolus is about 2 cm anterior to the lateral malleolus. Anatomic studies have shown that in any position, the tibial plafond covers only two thirds of the talar dome.
Portal placement is strongly influenced by the neurologic patterns of the lower extremity. Anteromedially, the saphenous nerve is on average 7 mm away for portal placement next to the tibialis anterior. The medial portal is always created first as it allows the easiest access and the least risk to neurologic structures (Fig. 48.1).
The anterolateral portal is established second and under direct visualization. The superficial peroneal nerve and its branches are at risk with this portal. The superficial peroneal nerve divides proximal to the ankle into the intermediate and medial dorsal cutaneous branches. The intermediate cutaneous branch passes superfi- cial to the inferior extensor retinculum, crosses anterior to the extensors to the fourth and fifth toes, and then runs toward the third interspace between toes 3 and 4. This is the nerve at greatest risk with anterior ankle arthroscopy (Fig. 48.1)
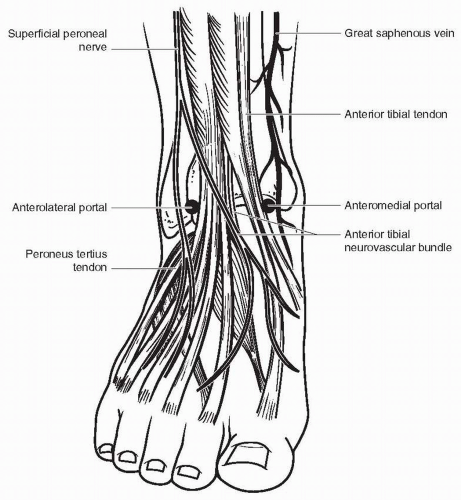 FIGURE 48.1 Portal Anatomy for ankle arthroscopy. |
 FIGURE 48.2 Noninvasive distraction strap. |
EQUIPMENT NEEDS AND PATIENT POSITIONING
Equipment needs specific for ankle arthroscopy include noninvasive distraction system, 3.5- or 2.0-mm 30-degree arthroscope, pressure inflow system or gravity flow system, arthroscopic shaver, and small joint arthroscopy instruments including graspers, currets, and awls.
The patient is placed supine on the operative table. A well-padded tourniquet is applied to the upper thigh and the operative extremity is placed in a thigh/knee holder with the knee flexed at approximately 45 to 60 degrees, with the foot and ankle resting approximately 3 to 4 in above the operating table. The holder is padded sufficiently to ensure there is no pressure on the peroneal nerve.
Distraction techniques facilitate the placement of the arthroscope and instruments into the tightly configured ankle joint. Noninvasive techniques involving straps, harnesses, and outriggers are the most commonly used distraction methods. These techniques minimize the risk of neurovascular injury and other complications (1) (Fig. 48.2).
After sterile preparation and drape of the ankle, a noninvasive ankle distractor strap is applied (Arthrex Inc, Naples, Florida). This may be safely distracted until the straps have significant tension. EMG studies have confirmed that neurologic change of the tibial nerve does not occur until there is 30 lb of tension (2). The manual strap does not allow this threshold to be reached.
PORTAL PLACEMENT
Anterior ankle arthroscopy is performed traditionally through two anterior portals. Neurologic structures are subcutaneous and portal placement is made in all cases by blunt dissection after the skin has been incised with the knife.
Related posts:
 Arthroscopic Management of Elbow Osteochondritis Dissecans Lesions
HAGL: Arthroscopic/Open
Meniscal Débridement
Aperture Fixation in Primary Arthroscopic Double-Bundle, Single-Bundle, and Single-Bundle-Augmented ACL Reconstruction
LCL/PLC Reconstruction
Cartilage Transplantation: Fresh Osteochondral Allograft
Arthroscopic Management of Elbow Osteochondritis Dissecans Lesions
HAGL: Arthroscopic/Open
Meniscal Débridement
Aperture Fixation in Primary Arthroscopic Double-Bundle, Single-Bundle, and Single-Bundle-Augmented ACL Reconstruction
LCL/PLC Reconstruction
Cartilage Transplantation: Fresh Osteochondral Allograft
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


