Figure 1.1 Schematic diagram of the respiratory system. See text for details. (With permission from Thibodeau GA, Patton KT, 1996. Anatomy and physiology, 3rd edn. Mosby, St Louis.)
The airways
The airways branch a total of 23 times, creating a tree-like structure that ends in the alveoli, where the exchange of oxygen (O2) and carbon dioxide (CO2) takes place (Fig. 1.2). The branches follow an irregular, dichotomous pattern in which each airway gives rise to two ‘daughter’ airways. The structure is irregular because the daughter branches may not be of equal size. The number of airways (N) in each generation (Z) is given by the equation N = Z2.
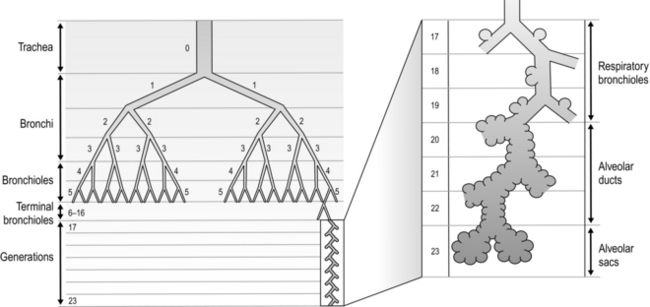
Figure 1.2 Diagram illustrating the branching structure of the lung airways. (With permission from Davies A, Moores C, 2010. The respiratory system. Churchill Livingstone, London, p. 15, Fig. 2.4.)
Air enters via the nose and mouth; then it travels into the pharynx, through the glottis and down the trachea. Next, the air travels into the right and left bronchi, and then through the branching structure of the remaining airways to the alveoli. The alveoli are collections of air sacs, similar to a bunch of grapes, which are surrounded by a dense network of capillaries (think of a bunch of grapes inside a net shopping bag; Fig. 1.1). The regions of the lung without alveoli (including the airways) are known as the conducting zone (branches 1–16), whilst the regions with alveoli are known as the respiratory zone (17–23), i.e., the zone where oxygen and carbon dioxide are exchanged (Fig. 1.2). From branch 17 onwards (respiratory bronchioles), the airways begin to display alveolar buds in their walls, and by branch 20 onwards virtually the entire airway is made up of alveoli (alveolar ducts). An important feature of the conducting airways is that the larger airways, such as the trachea, are reinforced with cartilage rings that help prevent collapse, whereas the walls of smaller airways contain no supporting skeleton. The small airways possess rings of smooth muscle that, when contracted, narrow the airways (bronchoconstriction). From branch 3 onwards, the airways are surrounded by lung parenchyma, and the elastic forces that operate to recoil the lung parenchyma help to tug the airways open during exhalation (airway tethering), with their radial traction (see section ‘Mechanics of breathing: Airway resistance’).
The alveoli
The branching structure of the lungs is an impressive work of evolution that has resulted in adult human lungs having a combined surface area of about 60 m2 (646 square feet), which is about the same as a singles badminton court and about 40 times the area of the skin (see Fig. 1.23). Why the need for such a huge area? Like so much of evolution, the respiratory system is a slave to the laws of physics. As will be described in detail in the next section, the exchange of oxygen (O2) and carbon dioxide (CO2) between the 300 million alveoli and the capillaries surrounding them occurs via passive diffusion. For this process to keep pace with the metabolic needs of the average person, especially during exercise, a vast surface area (number of alveoli and capillaries) is required for diffusion.
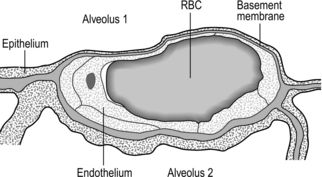
Figure 1.3 Drawing taken from an electron micrograph section of an alveolus showing the alveolar–capillary membrane. RBC = red blood cell. (With permission from Davies A, Moores C, 2010. The respiratory system. Churchill Livingstone, London, p.18, Fig. 2.9.)
However, this vast lung surface area would be of little use without the unique and intimate interrelationship that exists between the alveoli and their capillary network. Figure 1.3 illustrates the key feature of this structure, i.e., the minimal distance separating the alveolar air from the capillary blood. Note that on one side of the capillary the alveolar and capillary cells fuse to form a very thin septum, whilst on the opposite side of the capillary the septum is thicker, providing stability and resisting collapse.
The epithelial junctions are sufficiently leaky to allow the passage of water and solutes between the plasma and interstitial fluid, but not larger molecules, whose osmotic potential would cause oedema. These leaks also facilitate the movement of macrophages into the alveolus, where they scavenge foreign bodies (both organic and inorganic). Lining the alveoli and conducting airways is a fluid layer containing surfactant; the importance of this layer for diffusion and normal lung mechanics is explained in subsequent sections. Suffice to say, at this point, dissolving in this layer is one of the sequential steps that O2 and CO2 must pass through on their journey.
The blood vessels
The lungs have two blood supplies. The first arises from the right ventricle and carries deoxygenated blood via the pulmonary artery to the pulmonary capillaries, and thence the pulmonary vein back to the left atrium. The vessels follow the airways in connective tissue sheaths. Unlike the systemic circulation, pulmonary arterioles have very little smooth muscle. The capillaries traverse a number of alveoli before combining to form venules and veins. The latter do not follow the same branching route as the arteries, but instead run along septa that separate segments of the lungs.
The second circulation in the lungs arises from the aorta as the bronchial arteries, which meet the metabolic requirements of the conducting airways by perfusing the walls of the airways as far as the respiratory bronchioles (after which O2 requirements are met by alveolar gas exchange). Around one-quarter to one-third of the venous effluent from the bronchial circulation drains into the bronchial veins and thence to the right atrium. The remainder drains directly into the pulmonary veins via bronchopulmonary–arterial anastomoses, contributing to shunting of deoxygenated blood into the pulmonary veins. This shunt is the reason that the alveolar to arterial pressure difference for oxygen exists (see section ‘Gas exchange, Diffusion’ below).
The lymphatics
Lymph is a clear protein-containing liquid found in the extracellular and extravascular spaces. Were it not for the lungs’ lymphatic system, accumulation of lymph in the lungs would lead to pulmonary oedema and flooding of the alveoli. The system also has an important role in immune defence of the lungs. Lymph returns to the cardiovascular system through the right thoracic duct.
The nerves
The respiratory system is under both somatic and autonomic nervous control. The somatic system provides motor control of respiratory pump muscles, whereas the autonomic system provides both motor (efferent) and sensory (afferent) nerves to the lungs. For information on somatic nerve innervation of respiratory muscles see ‘The muscles’ (below).
Innervation of airways
The lungs are innervated exclusively by autonomic nerves, and there is no voluntary control of airway smooth muscle. Similarly, there is no sympathetic nervous control of airway smooth muscle; a sympathetic supply is present anatomically, but it appears to have no functional relevance for airway smooth muscle control. The only source of sympathetic bronchodilation is from circulating epinephrine (adrenaline) secreted by the adrenal gland, which acts on airway smooth muscle β2-receptors. In contrast, the parasympathetic supply to airway smooth muscle is extremely important. It also innervates mucous glands and blood vessels. The release of acetylcholine from these parasympathetic cholinergic fibres stimulates smooth muscle contraction, leading to bronchoconstriction, or bronchospasm. There is a continuous basal tone within the system, which produces a small amount of basal bronchoconstriction. This can be eliminated by circulating adrenaline, and is the reason that airway calibre increases for a short time after exercise in healthy people.
Secretory cells respond to parasympathetic stimulation by increasing the production of mucous glycoproteins, making secretions thicker, whereas sympathetic stimulation makes them more watery.
Innervation of blood vessels
The blood vessels of the lungs are innervated by both branches of the autonomic nervous system. In contrast to the airway smooth muscle, the most important functional connection is the sympathetic branch, which induces vasoconstriction. However, this activation appears to be associated with a limited range of situations, e.g., ‘fight or flight’ and heavy exercise.
The muscles
This section describes the anatomy and physiology of the muscles involved in breathing. This includes not only the respiratory pump muscles, but also the muscles in the upper airway that abduct the airway, and the trunk musculature, which is involved in maintenance of posture and stabilization of the pelvis and spine. The recognition that the entire trunk musculature has both respiratory and non-respiratory roles is an important concept to grasp, since this ‘multi-tasking’ has a profound bearing on the functional capacity of patients with respiratory muscle dysfunction. This section will provide an overview of how the respiratory muscles function, and interact, during exercise. It will also consider how their function can be limited by factors such as lung volume and air-flow rate. This knowledge will help to establish the rationale for a functional approach to training of the respiratory and other trunk muscles.
Respiratory pump muscles
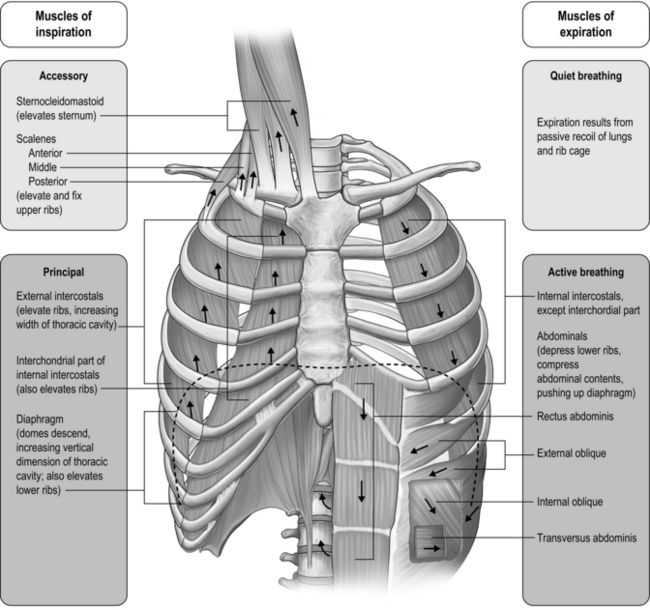
The respiratory pump muscles are a complex arrangement that form a semi-rigid bellows around the lungs. Essentially, all muscles that attach to the rib cage have the potential to generate a breathing action, but the principal muscles are shown in Figure 1.4. Muscles that expand the thoracic cavity are inspiratory muscles and induce inhalation, whereas those that compress the thoracic cavity are expiratory and induce exhalation. These muscles possess exactly the same basic structure as all other skeletal muscles, and they work in concert to expand or compress the thoracic cavity. The structure of the rib cage is described in the section ‘Gross structure of the respiratory system’ (below).
Inspiratory muscles
The principal muscle of inspiration is the diaphragm, a domed sheet of muscle that separates the thoracic and abdominal cavities. The diaphragm attaches to the lower ribs, as well as to the lumbar vertebrae. When the diaphragm contracts, the dome flattens, moving downward into the abdominal cavity like a piston (think of a syringe barrel). This movement increases the volume of the thoracic cavity, creating a negative pressure that is proportional to the extent of its movement, and thus, to the force of contraction. Diaphragm contraction also induces the lower ribs to move upward and forward, which also increases thoracic volume. The ribs move outward because the central tendon of the diaphragm (at the crown of the dome) pushes down onto the liver and stomach, which act as a fulcrum. This has the effect of raising the edges of the diaphragm, which are connected to the rib margins, forcing them upward and outward. When the diaphragm moves downward into the abdominal compartment, it also raises intra-abdominal pressure and assists the abdominal muscles in stabilizing the spine. Contraction of the diaphragm is controlled by a single nerve, the phrenic nerve, which originates from the 3rd to the 5th cervical vertebrae.
The muscles of the rib cage are known as the intercostal muscles because they are located in the space between adjacent ribs. Each space contains a layer of inspiratory and a layer of expiratory muscle fibres. The inspiratory intercostal muscles form the outer layer, and they slope downward and forward; contraction causes the ribs to move upward and outward, similar to the raising of a bucket handle. Contraction of these muscles also serves to stabilize the rib cage, making it more rigid, as well as bringing about flexing movements. The stiffening of the rib cage enables it to oppose the tendency to collapse slightly under the influence of the negative pressure generated by the movement of the diaphragm. Without this action, the rib cage would distort, and the action of the diaphragm would be less mechanically efficient, thus wasting energy. Intercostal muscle contraction also brings about stiffening of the rib cage during lifting, pushing and pulling movements, which makes the intercostal muscles important contributors to these actions. The nerves that control intercostal muscle contraction have their origin in the thoracic vertebrae (1st to 11th).
There are also muscles in the neck region with an inspiratory action. The scalene and sternocleidomastoid (sternomastoid) muscles are attached to the top of the sternum, upper two ribs and clavicle at one end; at the other end they are attached to the cervical vertebrae and mastoid process. When these muscles contract they lift the top of the chest, but the scalene muscles are also involved in flexion of the neck. The nerves that control these muscles have their origin in the cervical vertebrae.
Expiratory muscles
The principal muscles of expiration are those that form the muscular corset of the abdominal wall. The most well known and visible of these is the rectus abdominis; the other three muscles are less visible, but arguably more functionally important: the transversus abdominis and the internal and external oblique muscles. When these muscles contract, they pull the lower rib margins downwards and compress the abdominal compartment, raising its internal pressure. The pressure increase tends to push the diaphragm upwards into the thoracic cavity, inducing an increase in pressure and expiration. However, these muscles come into play as respiratory muscles only during exercise or forced-breathing manoeuvres; resting exhalation is a passive process brought about by the recoil of the lungs and rib cage at the end of inspiration (due to stored elastic energy).
The four abdominal muscles involved in breathing also have important functions as postural muscles: in rotating and flexing the trunk, and when coughing, speaking (or singing) and playing wind instruments. The compression and stiffening of the abdominal wall generated by contraction of the abdominal muscles also optimize the position of the diaphragm at the onset of inspiration. This also enhances spinal stability and postural control.
The rib cage also contains muscles with an expiratory action. These are the internal intercostal muscles, which slope backward; contraction causes the ribs to move downward and inward, similar to the lowering of a bucket handle. Both internal and external intercostal muscles are also involved in flexing and rotating of the trunk.
Other respiratory muscles
Theoretically, any of the muscles that attach to the rib cage have the potential to function as respiratory muscles. However, they do so only under extreme conditions such as after spinal injury, or during severe respiratory distress.
Functional properties of respiratory pump muscles
The functional properties of any given muscle are determined by the type of muscle fibres it contains. Human muscles have three main types of fibres, and most muscles contain a mixture of these, in differing proportions. The relative proportions of these three fibre types determine the properties of each muscle:
Type I and IIA fibres have a high oxidative capacity (ability to use oxygen to liberate energy) and a high to moderate density of blood capillaries (delivering oxygen). These fibres are also known as oxidative fibres, and they are capable of sustaining activity for prolonged periods without becoming fatigued.
It comes as no surprise to learn that the proportion of oxidative fibres (type I and type IIA) within the diaphragm and inspiratory intercostals is approximately 80% (Gollnick et al, 1972), whilst that of the expiratory intercostals is almost 100%. This compares with around 35–45% for limb muscles (Gollnick et al, 1972). The fibres of the abdominal muscles tend to be much more variable in their composition, reflecting the multiplicity of their roles. Another important factor determining muscle fatigue is its blood supply. Inadequate blood flow (ischaemia) not only limits oxygen delivery, it also limits the delivery of substrates and the removal of metabolic by-products, all of which can hasten fatigue. The diaphragm and rib cage muscles are supplied by numerous arteries. The diaphragm, for example, is perfused by three arteries, as well as benefiting from anastamoses that provide collateral sources of blood flow between arteries. The diaphragm also has an extremely dense capillary network and a capacity to increase its blood flow that exceeds that of limb muscles (Polla et al, 2004). The diaphragm maintains perfusion at contraction forces that occlude blood flow in limb muscles. This advantage derives from the fact that it is a thin sheet of muscle that produces a negative intrathoracic pressure during contraction; this pressure gradient maintains blood flow (Buchler et al, 1985). It has been suggested that this abundant and persistent arterial supply protects the diaphragm fibres from ischaemia (Hussain, 1996), providing resistance to fatigue.
In the past, the highly fatigue-resistant characteristics of the respiratory pump muscles contributed to a key assumption regarding the likelihood that the respiratory muscles contributed to exercise limitation. Physiologists assumed that the respiratory pump muscles, especially the diaphragm, were so well evolved from their continuous work that they were immune to fatigue. It wasn’t until the 1990s that this myth was finally shattered, when exercise-induced diaphragm fatigue was measured in healthy young athletes (see Ch. 3, section ‘Respiratory muscle involvement in exercise limitation, Healthy people’).
Upper airway muscles
The first question to address is why upper airway muscles are relevant to breathing. The simple answer is that, without them, upper airway resistance would be intolerable. During normal resting breathing, the vocal folds abduct during inhalation in order to widen the laryngeal glottic opening, permitting unobstructed air flow through the larynx (Brancatisano et al, 1984). This occurs via reflex activation of the posterior cricoarytenoid (PCA) muscle. Without this activity, the vocal folds would collapse across that laryngeal opening, causing an increase in resistance to upper airway flow and leading to increased breathing effort and dyspnoea. The strength of contraction of the PCA muscles has been shown to be proportional to factors that are associated with increased levels of respiratory drive, as well as the negativity of intrathoracic pressure (Suzuki & Kirchner, 1969). During vigorous breathing the action of the PCA is supplemented by contraction of the cricothyroid (CT), which acts to tension the vocal folds, increasing the anteroposterior dimension of the larynx (Hoh, 2005). Active closure of the vocal folds (adduction) is performed by the lateral cricoarytenoid muscle (LCA), thyroarytenoid (TA) and interarytenoid (IA), but only the PCA is involved in resting breathing. However, during tidal breathing most of the closure is brought about by relaxation of the PCA rather than by activation of the adductor muscles (Murakami & Kirchner, 1972). Transient, reflex modulation of the area of the laryngeal portion of the airway plays an important role in controlling breathing frequency, duty cycle and end-expiratory lung volume, as narrowing of the airway provides an important braking effect during expiration. Active adduction is associated with activities such as vocalization, coughing and straining.
The fibre type of human laryngeal muscles has not been studied nearly so extensively as limb muscles, but a number of key observations have been made with respect to the vocal fold abductors (PCA and CT). The PCA and CT contain around 66% and 45% type I fibres, respectively. The type II fibres of these muscles are limited to IIA and IIX, but the latter are very few in number. In common with limb muscles, PCA and CT appear to contain no IIB fibres (Hoh, 2005). The proportion of fast IIX fibres appears to be larger in the adductor muscles (TA and LCA), which probably imparts a higher velocity of shortening. This may be functionally important in their role as protectors of the airway (Li et al, 2004).
Because of its role in vocalization, the LCA has been studied in relation to its fatigability. Intramuscular EMG (electromyography) suggests that prolonged, loud vocalization exercises result in changes within the EMG that are consistent with the development of muscle fatigue (Boucher et al, 2006). Thus, it is reasonable to suggest that under similarly challenging conditions for abduction (e.g., vigorous breathing) PCA and CT might be similarly susceptible to fatigue. This is discussed in relation to exercise intolerance in Chapter 3 (section ‘Respiratory muscle involvement in exercise limitation’).
Gross structure of the respiratory system
The respiratory system is housed within the thoracic cavity, which is formed by the rib cage, vertebrae, sternum and diaphragm. Within the thorax there are three further cavities: the left and right pleural cavities and the mediastinum (Fig. 1.5).
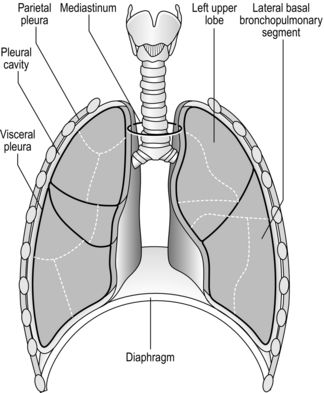
Figure 1.5 Gross anatomy of the lungs. (With permission from Davies A, Moores C, 2010. The respiratory system. Churchill Livingstone, London, p. 21, Fig. 2.12.)
The arrangement and movements generated by the respiratory muscles are described above (in ‘The muscles’). The skeletal structures that translate the muscle actions into movements are complex. The rib cage structure is such that the vertebral articulation of the ribs is higher than the sternal attachments; consequently, the ribs slope downwards anteriorly (Fig. 1.6).
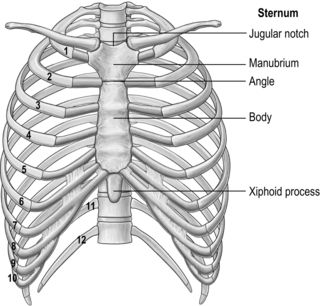
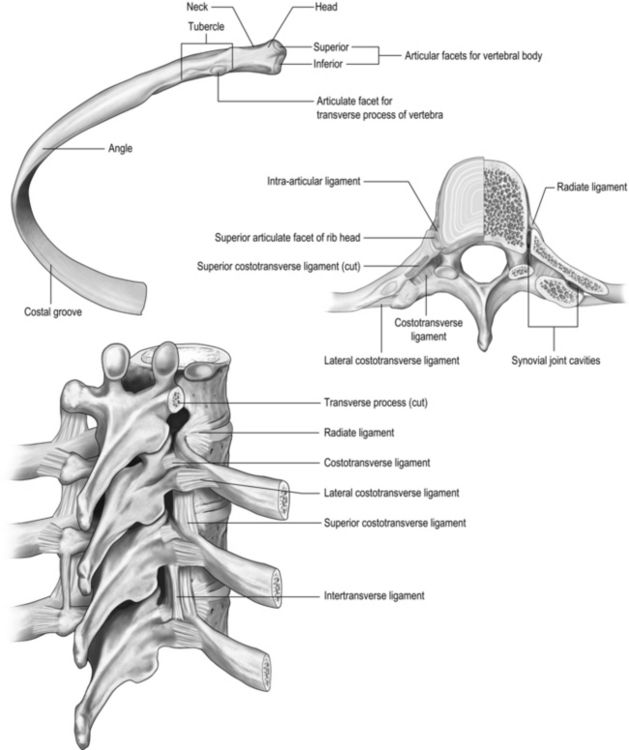
All 12 ribs articulate with the vertebrae, but only the first six connect individually to the sternum. Ribs 7–10 articulate with the lower sternum via a common cartilage, whilst ribs 11 and 12 have no anterior connections (‘floating ribs’). The head of most ribs articulates with the bodies of two adjacent vertebrae, whilst their tubercles articulate with the transverse process of one of these vertebrae. Nerves and blood vessels run in a channel on the underside of the ribs called the costal groove (Fig. 1.7).
The sternum has three parts: the manubrium, body and xiphoid process (xiphisternum). The junction between the manubrium and body of the sternum (sternal angle) is a useful anatomical landmark as it marks the level of the bifurcation of the bronchi (carina) and the second rib.
The process by which breathing is brought about is described in the sections ‘The muscles’ and ‘Mechanics of breathing’.
GAS EXCHANGE
Gas exchange is the process of transferring gases across the alveolar and capillary membranes and it requires both diffusion of gas and perfusion of blood. Diffusion is a passive process, and it is for this reason that the lungs have evolved the structure that we see in terrestrial mammals. The key features of the lungs’ passive diffusion system are:
It is easy to see how disease can affect all three of these factors, sometimes simultaneously, leading to a reduction in diffusing capacity.
The diffusion gradient is provided by the difference in partial pressure of the gases (P). The partial pressure of a gas is the proportion of the total barometric pressure that the gas contributes. For example, oxygen (O2) makes up 21% of the atmosphere; if barometric pressure is 760 mmHg (‘standard’ atmospheric pressure), the partial pressure of oxygen (PO2) is 20.93% of 760 mmHg, i.e., 159 mmHg. As air enters the alveolus, it is warmed and humidified, and water vapour contributes 47 mmHg pressure. Since total barometric pressure cannot change, the partial pressure of all of the other gases is reduced in proportion to the amount of water added. In the case of PO2 it is reduced to 149 mmHg:

However, the partial pressure of oxygen within the alveoli (PAO2) is not 149 mmHg because the inhaled breath is diluted by the air that remained in the lungs at the end of the previous breath (end-expiratory lung volume, EELV). The extent of the dilution depends upon a number of factors, including the EELV and the tidal volume (VT); typically PAO2 will be around 104 mmHg, giving a diffusion gradient of around 65 mmHg. Thus, VT affects both the flow of gas delivered to the alveoli (via the dead space to VT ratio; see ‘Lung volumes and capacities’, below), and the extent to which inspired PO2 (PIO2) is diluted by the EELV (inspired to alveolar gradient). This mixing of old and new gas also affects the diffusion gradient and exchange of CO2 because it has the effect of raising the partial pressure of CO2 (PCO2) in the alveoli (PACO2). Thus, it is easy to see how changes in breathing pattern can influence the driving pressure for gas exchange, leading to hypoxaemia and hypercapnia.
Under normal conditions, the movement of oxygen across the alveolar and capillary membranes is so efficient that the PO2 of the arterial blood leaving the lungs (PaO2) is very close to the PAO2. This is known as the a–A gradient, and an increase in this gradient is a sign that all is not well with the process of diffusion. Both the diffusion surface area and the diffusion distance can influence the a–A gradient, as well as how quickly the blood traverses the alveolar capillaries. Despite the diffusion gradient for CO2 being much smaller than that for O2 (around 5 mmHg compared with 65 mmHg, respectively), equilibration of pulmonary arterial and alveolar PCO2 is normally achieved. This is made possible by the fact that the solubility coefficient of CO2 is 23 times that of O2.
The reason that solubility affects diffusion efficiency is explained by Fick’s law, which describes the rate of movement of gases across a membrane:

where A is the diffusion area, S is the solubility coefficient of the gas, ΔC is concentration gradient for the gas (alveolar to pulmonary arterial), t is the membrane thickness (alveolar plus capillary), and MW is the molecular weight of the gas molecule (its physical size). Although CO2 is 23 times more soluble than O2, it has a larger MW making the actual diffusion rate 20 times greater. However, equilibrium between the alveolus and venous blood occurs at around the same time for both CO2 and O2 because of the lower ΔC and slower release of CO2 from the blood compared with that of O2. Importantly, the A in the Fick equation is not the lung surface area, but rather the surface area where there is both ventilation and perfusion, i.e., where air and blood meet. As will be explained in later sections, many factors can influence the distribution of both ventilation and perfusion, leading to ventilation / perfusion ( /
/  ) inequality, a reduction in A and an impairment of diffusion.
) inequality, a reduction in A and an impairment of diffusion.
Clinically, disease can affect the diffusion area, the concentration gradient and the diffusion distance (t). Problems with diffusion manifest first as hypoxaemia, because O2 can be brought closer to the limits of its diffusional capacity by disease. In contrast, hypercapnia is normally a sign of deficiencies of alveolar ventilation.
There is one final factor that influences the efficiency of gas exchange between alveolus and blood, viz., the characteristics of the blood supply to the alveolus, and in particular the time available for the diffusion and binding / release of O2 and CO2. Figure 1.8 is a diagrammatic illustration of the change in pulmonary blood gases as the blood traverses the lungs. Under resting conditions, the blood spends around 0.75 seconds in contact with the alveolar regions of the lung, during which time it will traverse a number of alveoli.
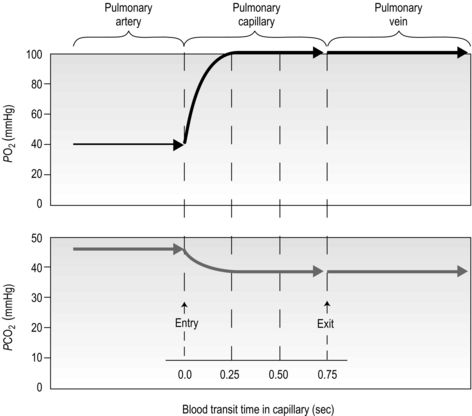
Figure 1.8 Equilibrium time for O2 and CO2 as blood traverses the alveolar capillaries under resting conditions. (With permission from Hicks GH, 2000. Cardiopulmonary anatomy and physiology. WB Saunders, Philadelphia, p. 365, Fig. 12-17.)
It is clear from Figure 1.8 that equilibration of both gases occurs early in the journey through the capillary, and that within 0.25 seconds diffusion ceases because there is no longer a gradient and exchange is complete. The only way to increase the exchange of gas is to increase the throughput of blood. In this scenario, gas exchange is perfusion limited. Many people find it hard to understand that, in healthy people at sea level, breathing more during exercise does not improve the amount of oxygen leaving the lungs; this is because it’s already ‘as good as it gets’. However, diffusion limitation can arise in healthy people under very specific conditions including: (1) exposure to high altitude (reducing the diffusion gradient), (2) during maximal exercise, when (a) cardiac output can be so high that blood traverses the lung capillaries before full equilibration can take place, (b) cardiac output can be so high that it outstrips the ability of the respiratory pump to deliver adequate alveolar ventilation (VA), (c)  /
/  inequality develops due to the mechanical effects of acute pulmonary oedema compressing alveoli and capillaries, and (d) the diffusion distance is increased by acute pulmonary oedema. Exercise-induced arterial hypoxaemia in healthy well-trained individuals at sea level is relatively rare and the specific contributions of the putative contributor remains incompletely understood (Guenette & Sheel, 2007).
inequality develops due to the mechanical effects of acute pulmonary oedema compressing alveoli and capillaries, and (d) the diffusion distance is increased by acute pulmonary oedema. Exercise-induced arterial hypoxaemia in healthy well-trained individuals at sea level is relatively rare and the specific contributions of the putative contributor remains incompletely understood (Guenette & Sheel, 2007).
In contrast to the rarity of diffusion limitation in healthy people, disease can inflict structural damage and functional changes that render affected individuals diffusion limited. For example:
 /
/  inequality due to disturbed lung mechanics and breathing pattern abnormalities
inequality due to disturbed lung mechanics and breathing pattern abnormalitiesPerfusion
In the previous section, we touched upon some perfusion-related factors that affected diffusion, e.g., diffusion area. Perfusion is such an important part of the gas exchange process that it merits specific consideration in relation to gas exchange; after all, under normal conditions, gas exchange is perfusion limited.
The pulmonary vasculature is supplied via a separate, low-pressure branch of the cardiovascular system. Deoxygenated blood is returned to the lungs via the right side of the heart and the pulmonary artery. The latter is the only artery in the body to carry deoxygenated blood, which is distributed to a huge capillary network within the lungs (Fig. 1.9).
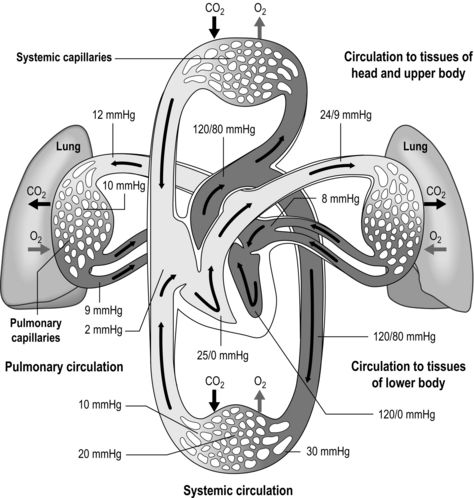
Figure 1.9 Schematic depicting pulmonary and systemic circulations and pressures. (With permission from Thibodeau GA, Patton KT, 1995. Anatomy and physiology, 3rd edn, Mosby, St Louis.)
As well as illustrating the flow of blood through both branches of the circulation, the diagram in Figure 1.9 also illustrates the pressures present within each part. Systolic / diastolic pressure in the pulmonary artery is around only 24 / 9 mmHg, compared with 120 / 80 mmHg in the aorta. The pulmonary circuit is at low pressure because of the thin, delicate walls of the capillary network, which minimizes the diffusion distance. Even small increases in pulmonary arterial pressure lead to fluid leakage and pulmonary oedema. Since the pulmonary circulation receives virtually the entire cardiac output, the fact that the pressures within it are low indicates that it has a low resistance. The reason for this low resistance is the extensiveness of its capillary network; as was described above, the capillary network can be thought of as a sheet of blood enveloping the alveoli.
Once gas exchange has taken place, the blood is returned to the left side of the heart to be distributed via the systemic circulation. In this way, the two parts of the circulation function in series, driven by a single pump. The difference in the pressures within the two sides of the circulation has a dramatic influence on the structure of the two sides of the heart: the muscular wall of the right ventricle is much thinner than that of the left, reflecting the lower resistance of the pulmonary circulation.
During exercise, cardiac output may increase from ~ 5 l·min−1 to ~ 25 l·min−1. This is accompanied by a small increase in systemic arterial blood pressure, and blood flow increases to exercising muscles because of vasodilatation in their vascular beds. In contrast, the pressure within the pulmonary circulation (receiving the same cardiac output) remains virtually unchanged during exercise. This is because the thin-walled pulmonary blood vessels distend, reducing pulmonary vascular resistance (PVR). In addition, there is recruitment of blood vessels in the pulmonary circulation; under resting conditions, not all blood vessels in the lungs are open fully (patent), but during exercise these vessels are recruited, and distended, stabilizing PVR.
One factor that has a strong influence upon the patency of pulmonary capillaries is alveolar pressure, which can compress the vessels. This increases their resistance, leading to redistribution of blood and heterogeneity of blood flow within the lungs. In addition, gravity, which also influences alveolar pressure (see ‘Pressures within the thorax’, below), has a potent influence upon blood flow distribution within the lungs. The effect is due to the hydrostatic pressure gradient that exists from the apex to the base of the lungs. It is very potent because pulmonary arterial pressure is so low that it is only just sufficient to pump blood to the lung apices. Perfusion pressure at the base of the lungs is equivalent to pulmonary arterial pressure, plus the hydrostatic pressure difference between the heart and base of the lungs. At the apex, perfusion pressure is equivalent to pulmonary arterial pressure, minus the hydrostatic pressure difference between the heart and apex of the lungs. This means that blood flow is distributed preferentially to the base of the lungs. As will be described in a later section (‘Pressures within the thorax’), ventilation is also distributed preferentially to the base of the lungs. However, the relative distribution of ventilation and perfusion is imperfect; there is around a three- to four-fold difference in ventilation from apex to base, compared with only a 16-fold difference in perfusion. Accordingly, there is a gradient of ventilation perfusion ratios ( /
/  ), and gas exchange, throughout the lungs. These variations in gas exchange also lead to local variations in the alveolar gas partial pressures. These phenomena are summarized in Figure 1.10.
), and gas exchange, throughout the lungs. These variations in gas exchange also lead to local variations in the alveolar gas partial pressures. These phenomena are summarized in Figure 1.10.
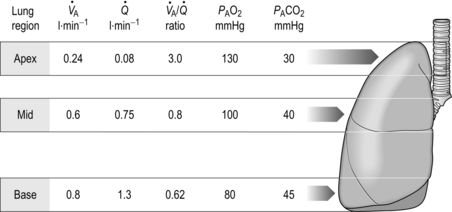
Figure 1.10 Variations in alveolar ventilation ( A) and perfusion (
A) and perfusion ( ). (With permission from Hicks GH, 2000. Cardiopulmonary anatomy and physiology. WB Saunders, Philadelphia, p. 352, Fig. 12-9.)
). (With permission from Hicks GH, 2000. Cardiopulmonary anatomy and physiology. WB Saunders, Philadelphia, p. 352, Fig. 12-9.)
In summary, the factors influencing blood-flow distribution in the lungs include:
There are three more influences upon the pulmonary circulation that need to be considered: (1) the direct effect of hypoxia upon pulmonary blood vessels, (2) the effect of humoral substances (e.g., histamine) and (3) neural influences:
 /
/  for the lung as a whole. In patients with conditions such as COPD (chronic obstructive pulmonary disease), in whom alveolar hypoxia is a chronic phenomenon, HPV can result in extensive pulmonary vasoconstriction. This increases PVR and the load placed upon the right side of the heart. As a result, both pulmonary oedema and right heart failure (cor pulmonale) can ensue.
for the lung as a whole. In patients with conditions such as COPD (chronic obstructive pulmonary disease), in whom alveolar hypoxia is a chronic phenomenon, HPV can result in extensive pulmonary vasoconstriction. This increases PVR and the load placed upon the right side of the heart. As a result, both pulmonary oedema and right heart failure (cor pulmonale) can ensue.OXYGEN AND CARBON DIOXIDE TRANSPORT
The primary function of the respiratory system is the delivery of oxygen (O2) and removal of carbon dioxide (CO2) from the body. Oxygen is required to liberate energy from food, and CO2 is a by-product of this chemical process. As we learnt in the previous section, the movement of O2 and CO2 occurs via a process of passive diffusion that is driven by the presence of concentration gradients. Oxygen moves down a concentration gradient from the alveoli to the cells, whilst CO2 moves down a gradient from the cells to the alveoli. The gases are transported between the lungs and tissues via the medium of the blood, which contains specialized cells that have evolved to make this process extremely efficient. The red blood cells (RBCs), or erythrocytes, play an important role in the transport of both O2 and CO2, but not before the gases have dissolved briefly in the other important constituent of blood, viz., the plasma. The ability of the plasma to transport O2 in simple solution is extremely limited (3 ml·l−1), but evolution has provided an answer to this limitation in the form of haemoglobin (Hb). This important molecule is contained within the RBCs, and without it multicellular animals could not have evolved beyond a worm-like collection of cells. Haemoglobin also plays a role in CO2 transport, but it is only one of a number of ways in which CO2 is transported. The addition of CO2 to the blood must be regulated very carefully because it forms carbonic acid in solution. Hence, the blood contains a number of protein buffers as well as bicarbonate and phosphate that minimize changes in blood pH. As we will see in the section on acid–base balance, breathing has a vital role to play in pH homeostasis.
Oxygen transport
Without haemoglobin, the O2-carrying capacity of the plasma (3 ml·l−1) would necessitate a blood flow through the lungs of 40 l·min−1 in order to meet a typical resting O2 requirement of ~ 250 ml·min−1. When one considers that the maximal cardiac output of a highly trained young person is only around 30 l·min−1, it is easy to see the need for Hb in an animal the size of a human being.
The molecule Hb allows the blood to carry around 20 ml·l−1, which means that a normal resting cardiac output of 5 l·min−1 can deliver the required 250 ml·min−1 for resting metabolism. Each Hb molecule consists of a protein (globin) and haem (an iron-containing pigment). Globin consists of four protein chains (two α and two β), each connected to a haem group; thus each Hb contains four protein chains and four haem groups (Fig. 1.11). Each of the four haem groups can bind to one O2 molecule, so conceptually each Hb molecule has four ‘hooks’ available to attach to four molecules of O2.
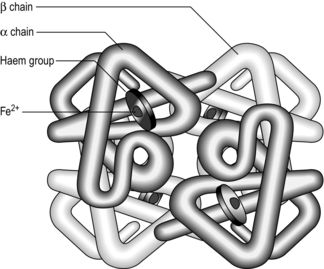
Figure 1.11 Schematic of the haemoglobin molecule. (With permission from Davies A, Moores C, 2010. The respiratory system. Churchill Livingstone, London, p. 101, Fig. 8.1, top.)
Oxygen binds to the haem groups of Hb in a reversible reaction, that is driven towards the formation of oxyhaemoglobin (HbO2) by high PO2, and towards deoxyhaemoglobin (Hb) and O2 by low PO2:

Thus, the chemical properties of Hb promote the loading of O2 (oxygenation) in the high-PO2 environment of the lungs, and unloading of O2 by the low-PO2 environment in the tissues. The binding of O2 to a haem group changes the shape of its protein chain, making it easier for the next O2 to bind to an adjacent haem group, and so on. This property is what gives the oxyhaemoglobin dissociation curve its characteristic sigmoid shape (Fig. 1.12).
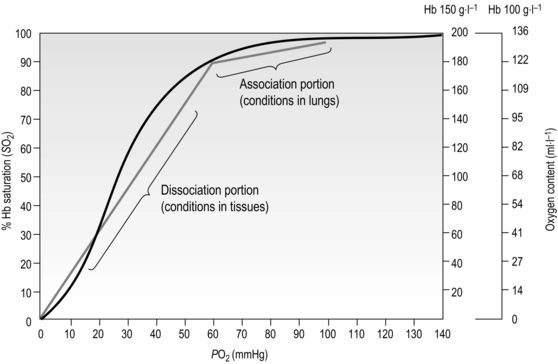
Figure 1.12 Association and dissociation of oxygen from haemoglobin (Hb). Note that the blood of a patient with anaemia, who may have a Hb content of only 100 g·l−1, can carry only 136 ml·l−1 of O2 (O2 content) when fully saturated, compared to an O2 content of 175–200 ml·l−1 in someone with normal Hb content of 150 g·l−1; but both people may have fully saturated Hb. (With permission from Beachey W, 1998. Respiratory care anatomy and physiology, 2nd edn. Mosby, St Louis, p. 140, Fig. 8.5.)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


