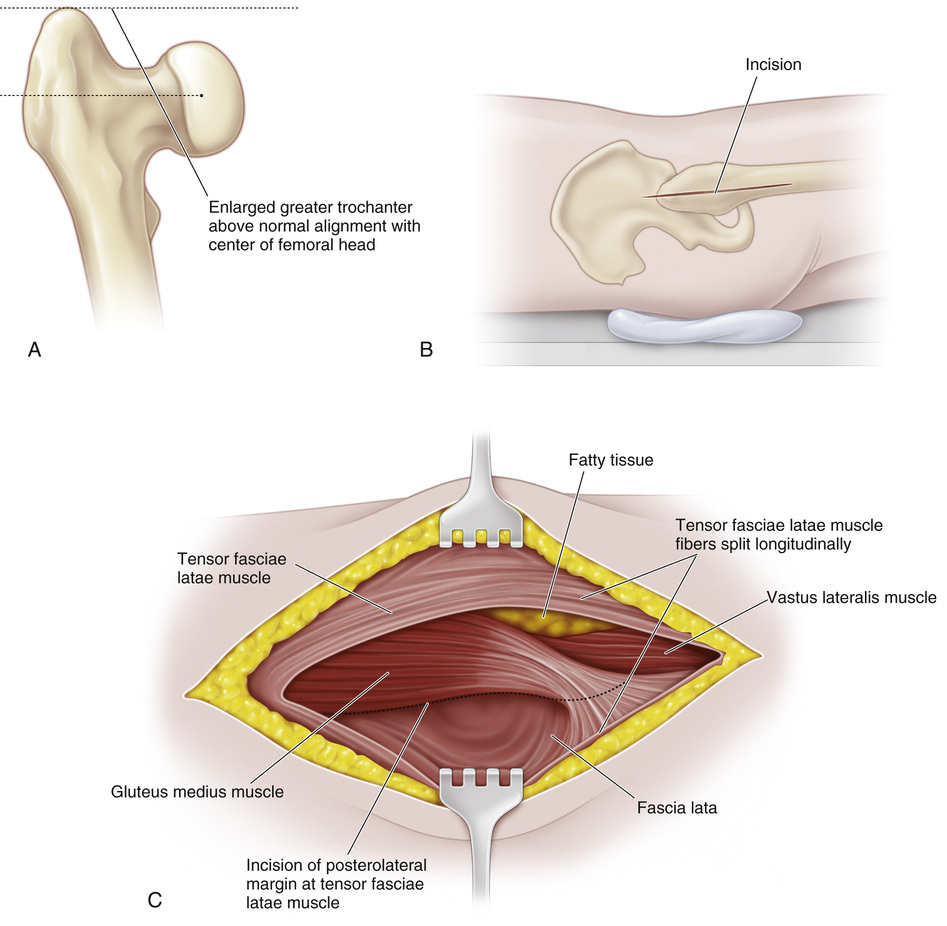
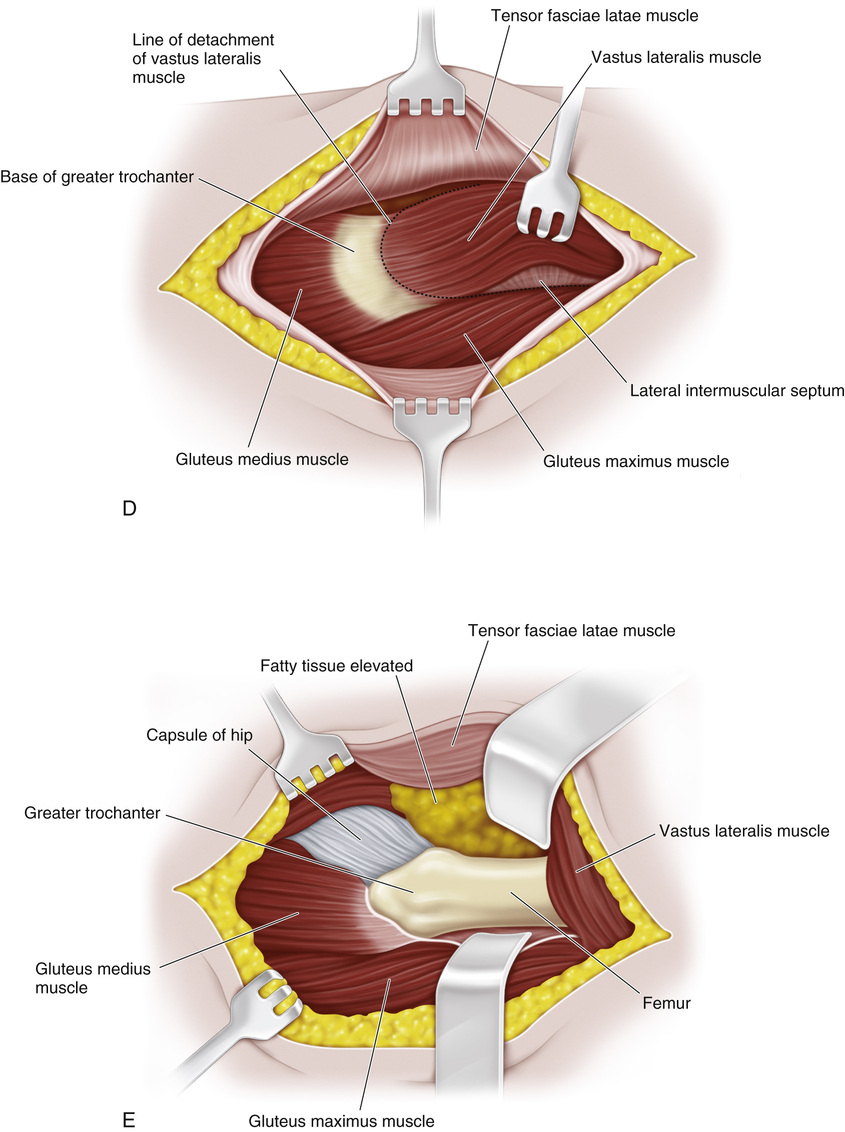
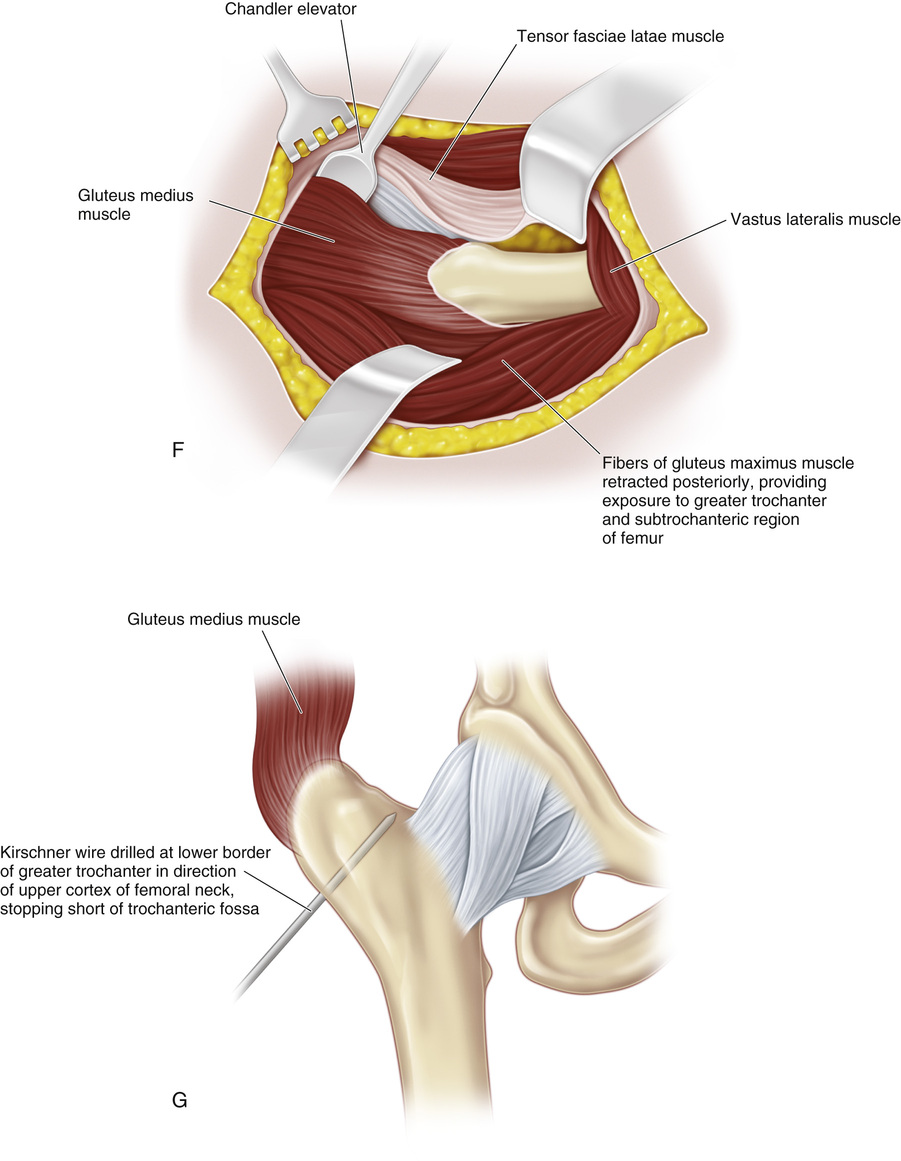
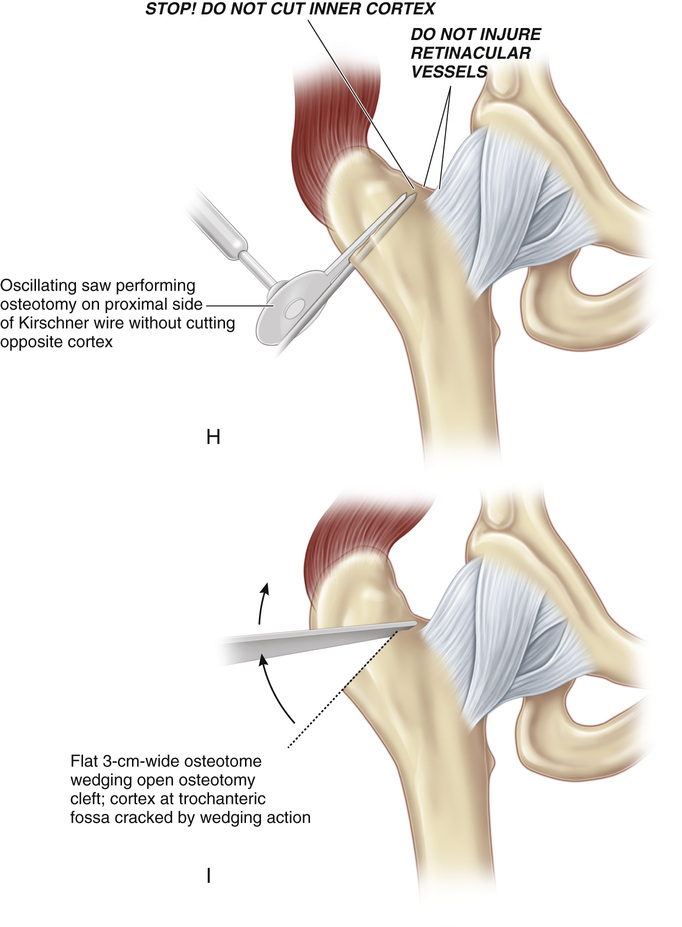
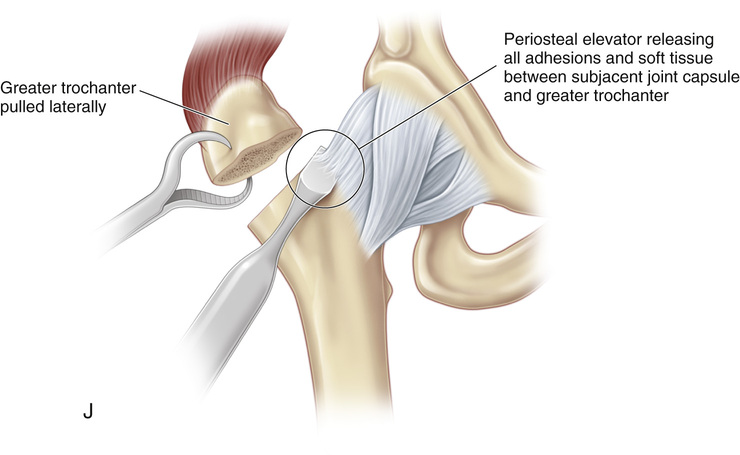
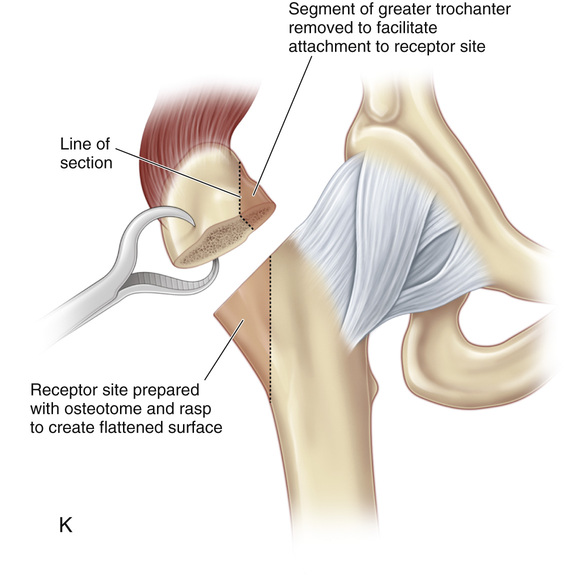
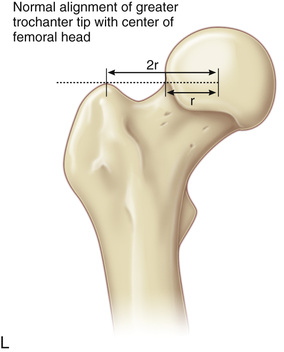
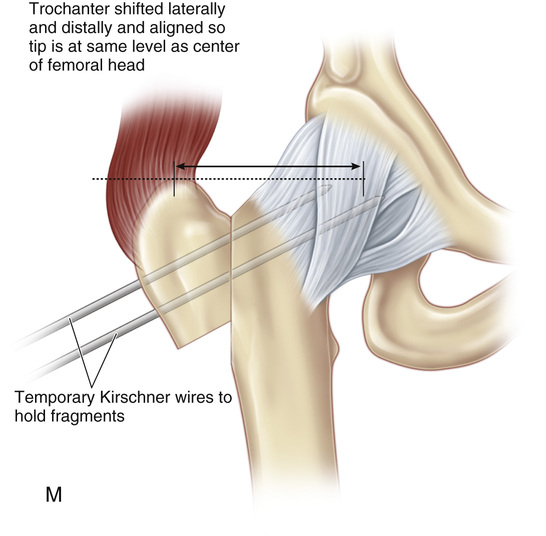
A and B, The patient is placed on the fracture table with the affected hip in a neutral position with regard to adduction and abduction and in 20 to 30 degrees of medial rotation to bring the greater trochanter forward to facilitate exposure. The opposite hip is placed in 40 degrees of abduction. Image-intensifier anteroposterior fluoroscopy is used to show the femoral head and neck, the greater trochanter, and the upper femoral shaft. The hip should be rotated medially so that the greater trochanter is seen in profile and not superimposed on the femoral neck. It is crucial to see the trochanteric fossa. The affected hip and the upper two thirds of the thigh are prepared and draped in the usual manner. A straight, lateral, longitudinal incision is made from the tip of the greater trochanter and extended distally for 10 cm. The subcutaneous tissue is divided in line with the skin incision. C, The fascia lata is split longitudinally in the direction of its fibers. D and E, The vastus lateralis is detached proximally from the abductor tubercle by a proximally based horseshoe-shaped incision and elevated subperiosteally from the femoral shaft for 5 to 7 cm. The vastus lateralis should be elevated over its entire width. F, The anterior border of the gluteus medius is identified, and a blunt elevator retractor is introduced beneath its deep surface; it is pointed in the direction of the trochanteric fossa. G, At this time, to orient the plane of the trochanteric osteotomy properly, a smooth Kirschner wire is inserted at the level of the abductor tubercle; it points to the trochanteric fossa along a line that is continuous with the upper cortex of the femoral neck. Radiography with image intensification verifies the proper level and depth of the guide wire. The point of the Kirschner wire must not protrude through the medial cortex into the trochanteric fossa. H, A blunt, flat retractor is placed beneath the posterior border of the greater trochanter to protect the soft tissues. The previously applied anterior retractor protects the soft tissues ventrally. With a 2- to 3-cm-wide reciprocating saw, the greater trochanter is divided in the anteroposterior direction, following the proximal border of the Kirschner wire. The cut is stopped 3 mm short of the medial cortex of the trochanteric fossa. Injury to the vessels in the trochanteric fossa must be avoided to prevent necrosis of the femoral head. I, Next, a 3-mm-wide flat osteotome is driven through the osteotomy cleft, and the osteotomy site is wedged open by moving the handle of the osteotome craniad. By applying leverage with the osteotome in the cleft, the operator produces a greenstick fracture of the medial cortex. J, A large periosteal elevator is placed deep into the osteotomy cleft; this cleft is opened up medially by gently levering the handle up and down. The trochanteric fragment is lifted superolaterally with a Lewin bone clamp, and adhesions between the joint capsule and the medial aspect of the greater trochanter are released. This must be done very carefully to avoid injuring retinacular blood vessels in the capsule. Do not fracture the greater trochanter. Mobilization is sufficient when, with lateral and distal traction placed on the greater trochanter, the muscle response is elastic; if there is still muscle resistance, it means that further adhesions are present that must be freed. K, After sufficient mobilization of the greater trochanter, the recipient site on the lateral surface of the upper femoral shaft is prepared with a curved osteotome to create a flattened surface. The surgeon should not remove too much bone laterally. Next, the greater trochanter is displaced distally and laterally; with excessive femoral antetorsion, it may be moved slightly forward. If additional distal advancement is desired, the hip may be abducted on the fracture table. L and M, The trochanter is held in the desired position and temporarily fixed to the femur with two threaded Kirschner wires of adequate size that are drilled upward and medially. At this point, the accuracy of the position of the greater trochanter is verified with image-intensifier radiography. As stated previously, the tip of the greater trochanter should be level with the center of the femoral head and at a distance from it of two to two-and-one-half times the radius of the femoral head. If there are problems with proper visualization, a long Kirschner wire is placed horizontally and parallel to both anterior superior iliac spines so that it crosses the center of the femoral head; the position of the tip of the greater trochanter is then checked. N, Before osteosynthesis, the gluteal muscle is split in the direction of the fibers to expose the bone and to avoid muscle necrosis. The greater trochanter is fixed to the lateral surface of the upper femur with two lag screws (each equipped with a washer), which are directed medially and distally at 45-degree angles to counteract the pull of the hip abductors. For large trochanters, 6.5-mm cancellous screws with drill bits of appropriate size are used; with smaller trochanters, 3.2-mm screws are used. The outer cortex of the greater trochanter may be overdrilled. The tapping of the outer cortex is optional. The washers increase the surface area, help the operator to avoid cutting through the cortex, ensure more secure fixation, and allow for early motion. After both screws are inserted, the initial Kirschner wires are removed. O, Alternatively, fixation can be achieved with two heavy, threaded Kirschner wires directed medially and upward. The resultant pull of the hip abductors through the direction of the wires provides a force that will compress the greater trochanter against the lateral surface of the femur. We do not recommend internal fixation with the use of this method because screw fixation is more stable. However, in an obese or uncooperative patient, threaded Kirschner wires may be used in addition to screw fixation. Alternatively, a tension wire band may be used as described in Procedure 8 on page 29, “Lateral Advancement of the Greater Trochanter.” P, Final intraoperative radiographs are obtained to ensure that the trochanter has been advanced to the desired site. Next, the detached origin of the vastus lateralis is firmly sutured to the tendinous insertion of the gluteus medius and minimus muscles. This tension-band suture absorbs the pull of the hip abductors and reinforces the internal fixation of the greater trochanter. A suction drain is inserted, and the remainder of the wound is closed in routine fashion. The skin closure is subcuticular.
Distal and Lateral Transfer of the Greater Trochanter
Operative Technique
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


