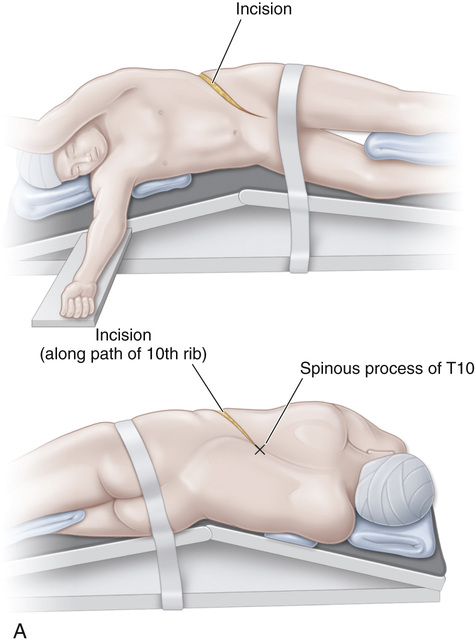
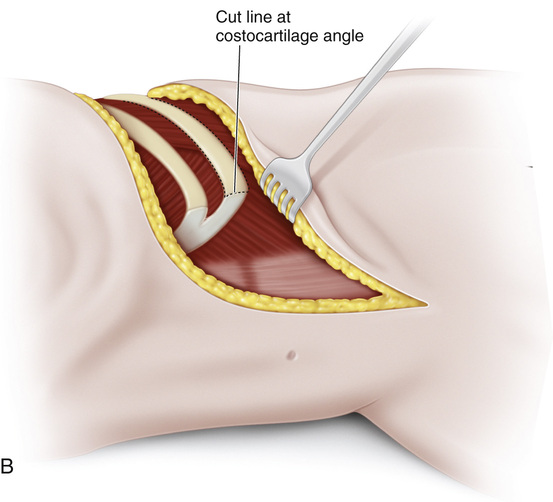
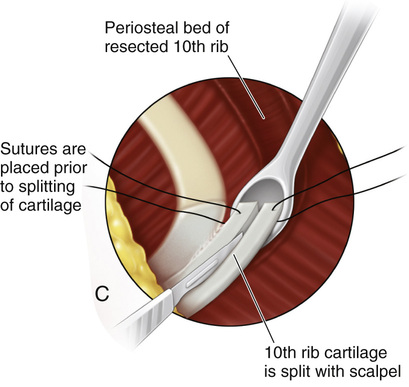
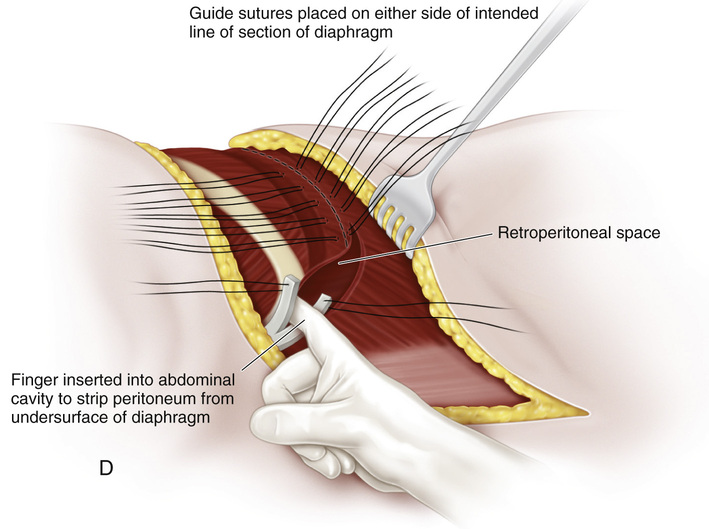
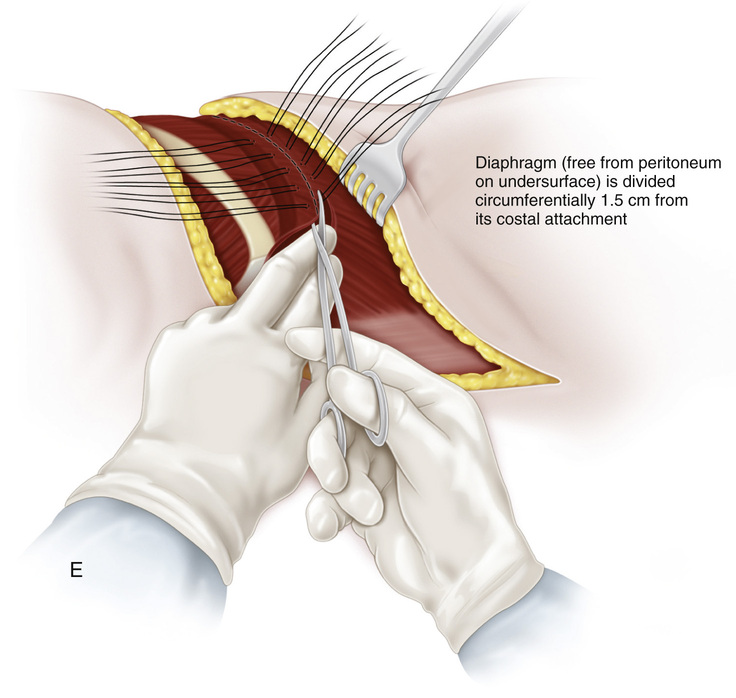
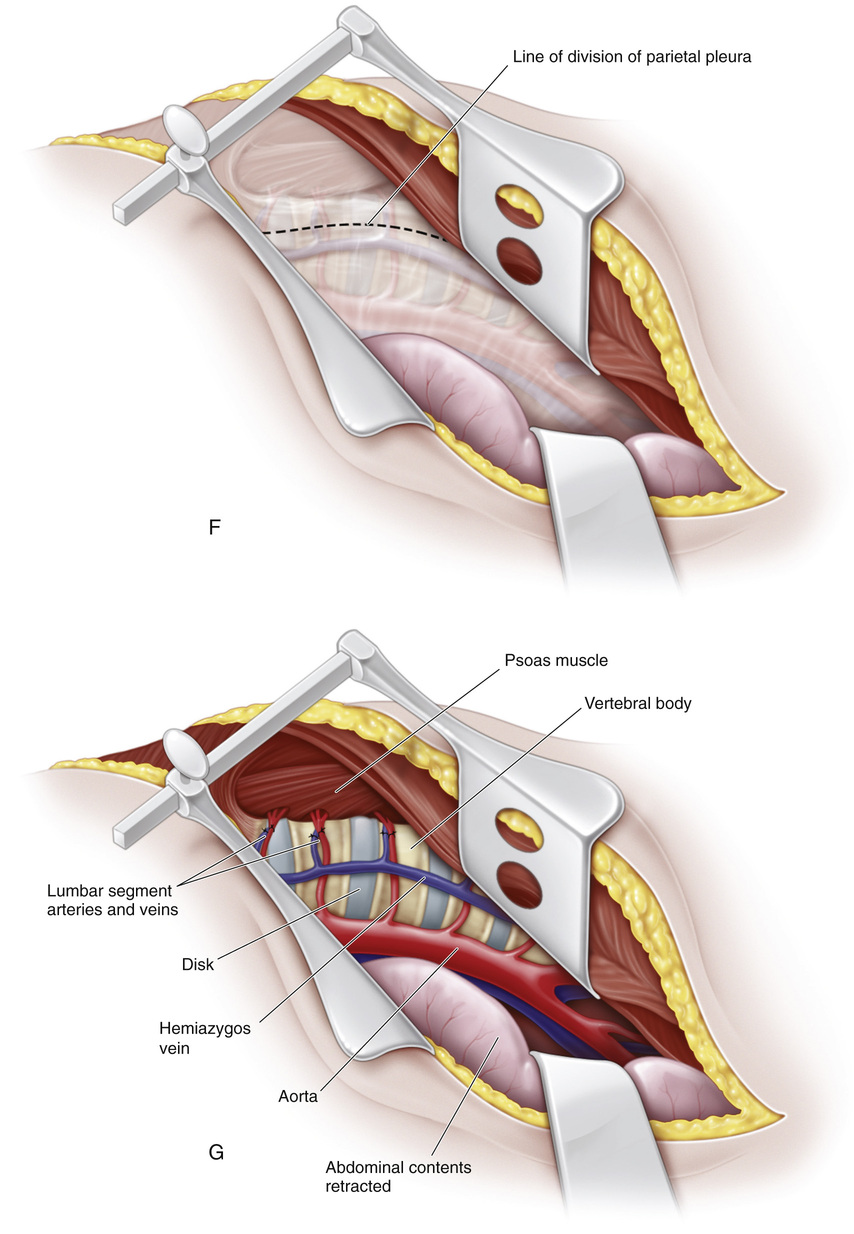
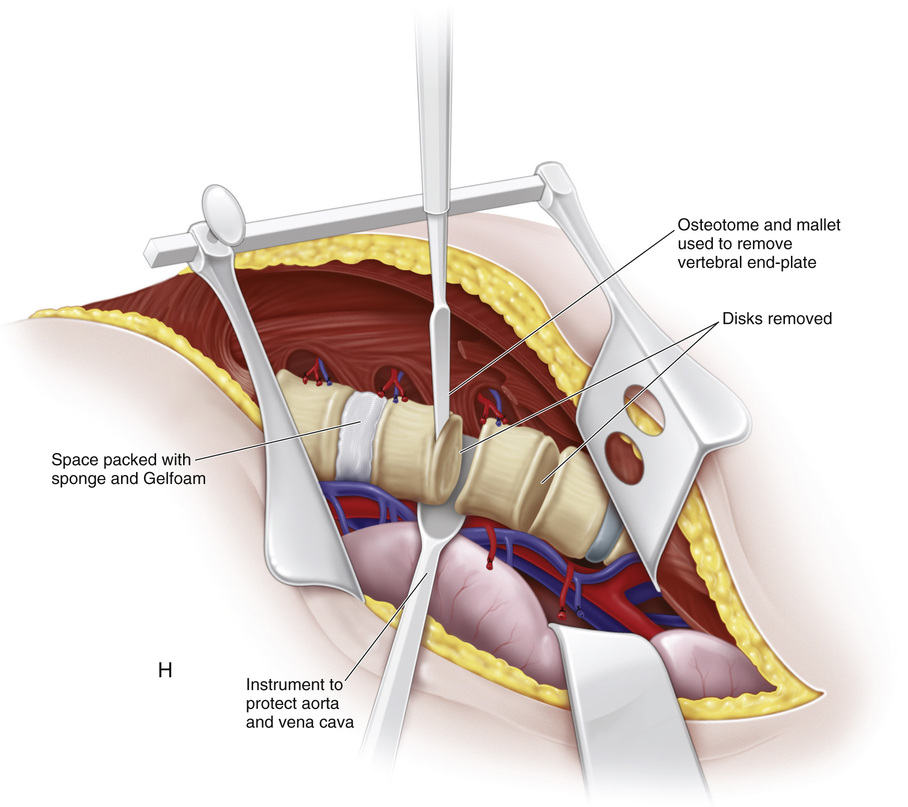
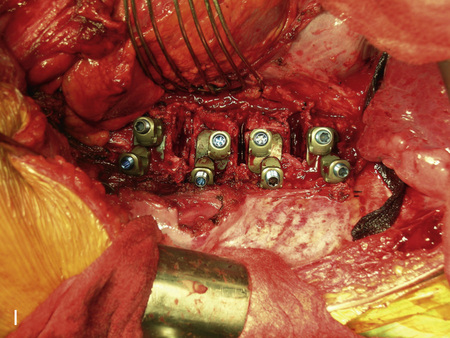
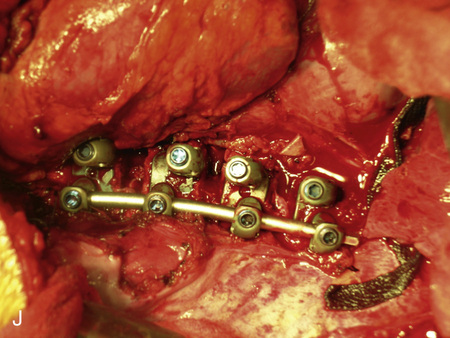
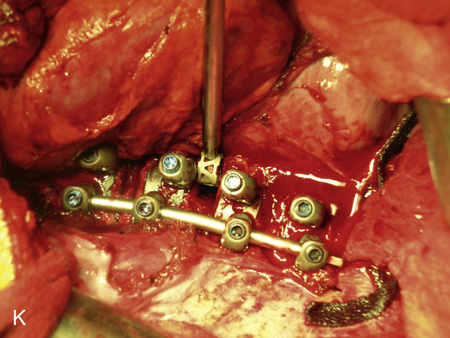
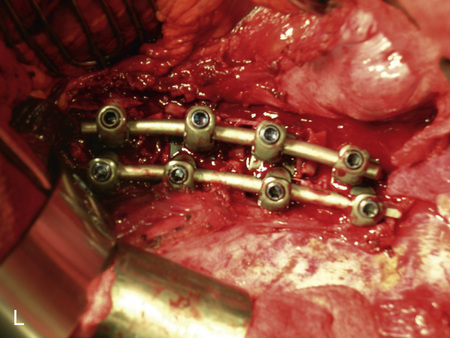
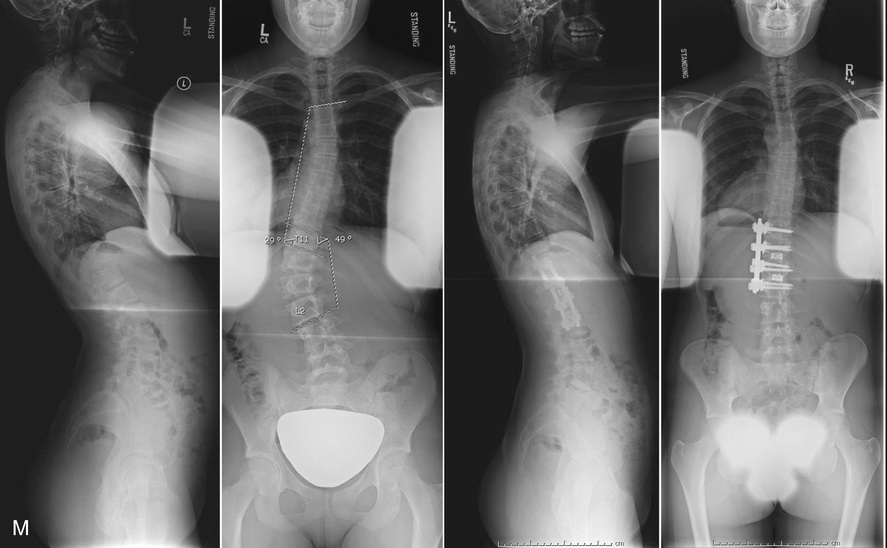
In this plate the thoracoabdominal approach for exposure of the lower thoracic and lumbar spine is described. A, Positioning. Under the direction of the surgeon, the patient is placed in the lateral decubitus position (the convexity of the curve is upward). A roll is placed under the axilla of the dependent arm. The body is supported with a deflatable beanbag. The upper part of the arm is flexed forward and slightly abducted. The operating table may be temporarily flexed (at the apex of the scoliosis) to facilitate excision of the intervertebral disks. Approach. It will be necessary to remove a rib for exposure of the spine. Ideally, the rib that is removed is the one immediately cephalad to the uppermost vertebral body requiring instrumentation. For instrumentation between T11 and L3, removal of the tenth rib allows adequate exposure. Skin incision. The incision begins lateral to the spinous process of T10 (or T9) and extends along the course of the tenth rib to the costocartilaginous junction and then across the upper part of the abdomen to the lateral edge of the rectus abdominis. Here, it turns distally toward the symphysis pubis and stops at the level of the umbilicus. B, The tenth rib is freed subperiosteally, divided at its costocartilaginous junction, and removed. This creates a larger working aperture and provides a source of autogenous bone graft. C, Once the costal cartilage of the tenth rib is split, the retroperitoneal space is identified and entered. D, Using blunt finger dissection, the operator separates the peritoneum from the inferior aspect of the diaphragm. Once freed, the viscera lie safely away from the vertebral bodies. Identification sutures are placed on either side of the intended line of division of the diaphragm, which is ½ to ¾ inch from its periphery. Placement of several of these sutures facilitates proper closure of the diaphragm later. E, The diaphragm is sectioned from its costal attachments. F, Next, the parietal pleura is incised along the thoracic vertebral bodies that are to be included in the fusion. G, In the lumbar region, the psoas muscle is gently elevated off the vertebral bodies and intervertebral disks and retracted posteriorly. The segmental vessels are ligated in the middle of each vertebral body included in the fusion. The aorta and vena cava are protected with retractors, and the anterior longitudinal ligament is partially excised with a sharp scalpel. Each disk within the levels selected for fusion is removed with various rongeurs and curets. H, With a curet or sharp osteotome and mallet, the operator removes the vertebral cartilaginous end-plates and retained pieces of disk. For correction of kyphosis, most of the annular ligamentous tissue down to the posterior longitudinal ligament is removed. For scoliosis, however, the outer annular fibers need not be fully removed. The disk spaces are then temporarily packed with Gelfoam to minimize bleeding. If the operating table was flexed to facilitate excision of intervertebral disks, it should be flattened at this time. I, Following complete disk excision, the dual screws are placed via some guidance with a dual-headed staple. Retraction of the abdominal contents is seen at the top of the photo. J, The precontoured posterior rod has been placed and a rod rotation maneuver was performed to correct the scoliosis and improve the lumbar lordosis. K, Following rod rotation, anterior structural support is placed to maintain the lumbar lordosis, to assist in correction of the coronal plane deformity, and to increase the stiffness of the construct. L, Final construct after the anterior rod has been placed. M, Preoperative and 2-year radiographs following anterior spinal fusion and instrumentation with a dual-rod system and anterior autologous rib bone graft.
Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Operative Technique
Related posts:
 23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


