Pemberton Osteotomy
(see Video 4) 
The skin of the affected side of the abdomen and pelvis and the entire lower limb are prepared with the patient lying on his or her side, and the patient is draped to allow for free hip motion during surgery. Next, the patient is placed completely supine. The operation is performed on a radiolucent operating table. It is imperative to have image-intensification fluoroscopic and radiographic control.
Operative Technique
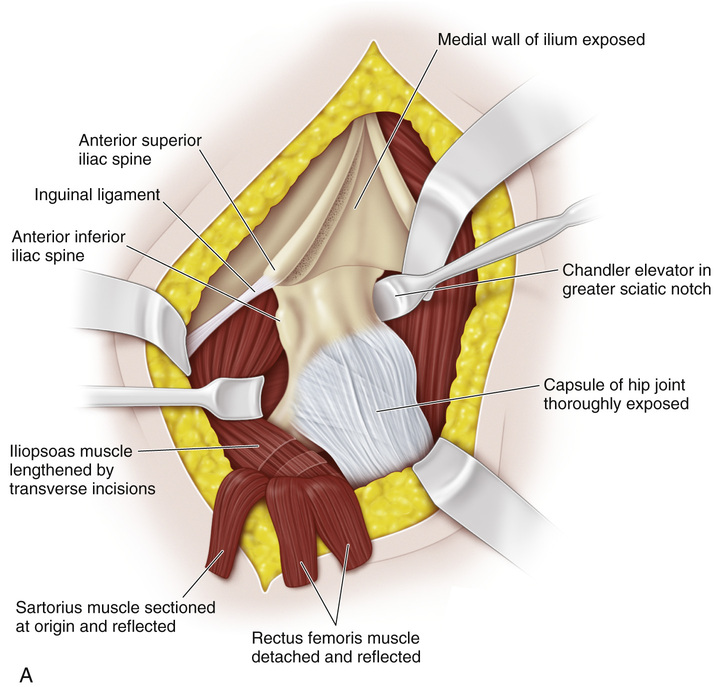
A, The medial and lateral walls of the ilium and the hip joint are exposed through an anterolateral iliofemoral approach. The cartilaginous apophysis of the ilium is split in accordance with the Salter technique. The sartorius muscle is sectioned at its origin from the anterior superior iliac spine, tagged with 2-0 Mersilene suture, and reflected distally. Both heads of the rectus femoris are divided at their origin and reflected. The iliopsoas tendon is lengthened by transverse incisions, and the Pemberton iliac osteotomy lengthens the pelvis. Division of the psoas tendon (not the iliacus muscle) decreases the pressure over the femoral head.
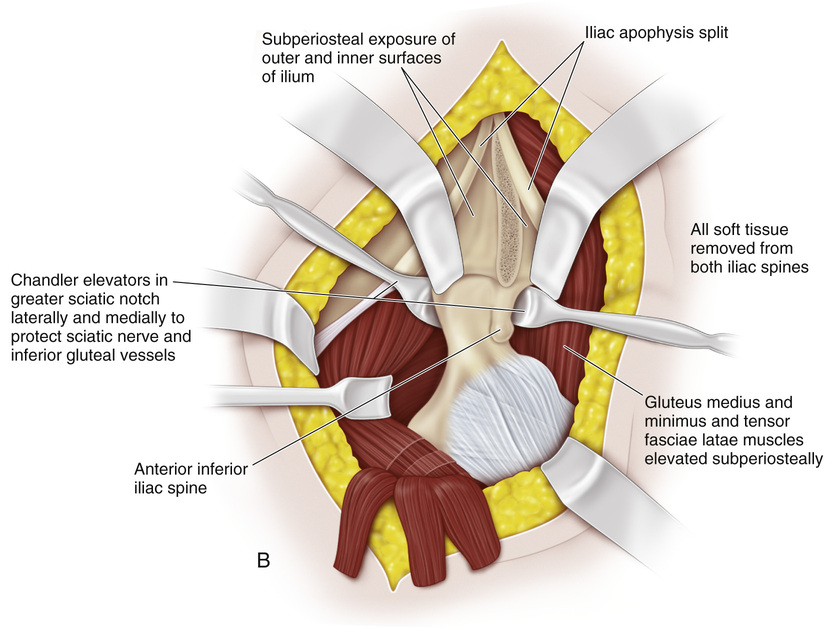
B, The ilium is exposed subperiosteally all the way posteriorly. The interval between the greater sciatic notch and the hip joint capsule posteriorly is developed gently and cautiously. The periosteal elevator meets resistance at the posterior limb of the triradiate cartilage. Chandler elevator retractors are placed in the greater sciatic notch medially and laterally to protect the sciatic nerve and the gluteal vessels and nerves. On the inner wall of the pelvis, the periosteum and the cartilaginous apophysis may be divided anteriorly to posteriorly at the level of the anterior inferior iliac spine as far as the sciatic notch; this will facilitate the opening up of the osteotomy.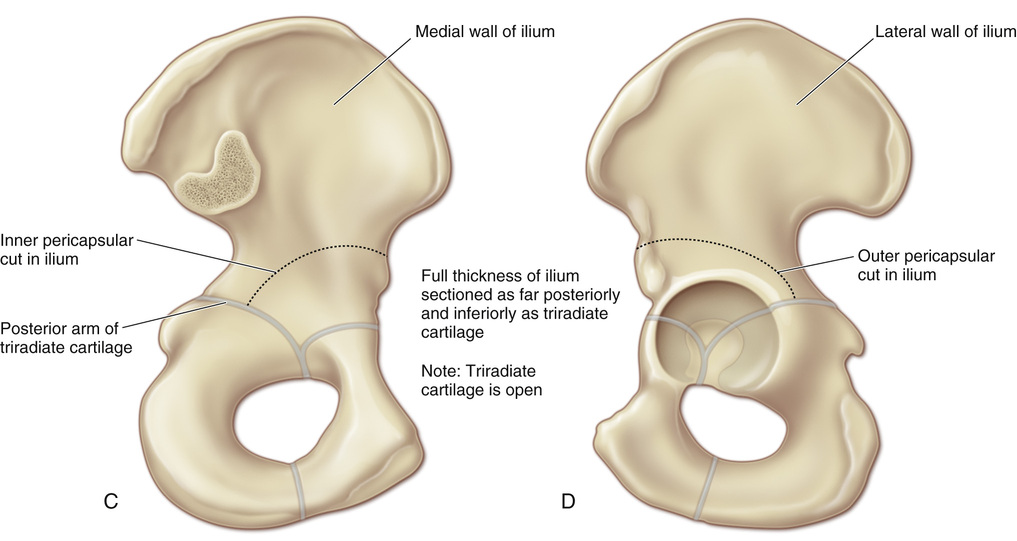
C to E, The osteotomy is first performed on the outer table of the ilium. The cut is curvilinear, and it describes a semicircle around the hip joint on the lateral side at a level that is 1 cm above the joint, between the anterior superior and anterior inferior iliac spines. It is best to mark the line of the osteotomy with indelible ink. The sharp edge of a thin osteotome is used to make the cut. The osteotomy ends at the posterior arm of the triradiate cartilage; this is most difficult to see if the exposure is inadequate. Image-intensification fluoroscopy helps to determine the terminal point of the cut at the triradiate cartilage, which is anterior to the greater sciatic notch and posterior to the hip joint margin. The next cut is made on the inner wall of the ilium, and it should be inferior to the level of the outer cut. The more distal the level of the inferior cut, the greater the extent of lateral coverage. If more anterior than superior coverage is required, then the medial and lateral cuts in the ilium are parallel. The importance of sectioning the ilium as far posterior and inferior to the triradiate cartilage as possible cannot be overemphasized. It is vital to not violate the articular cartilage of the acetabulum and enter the hip joint.
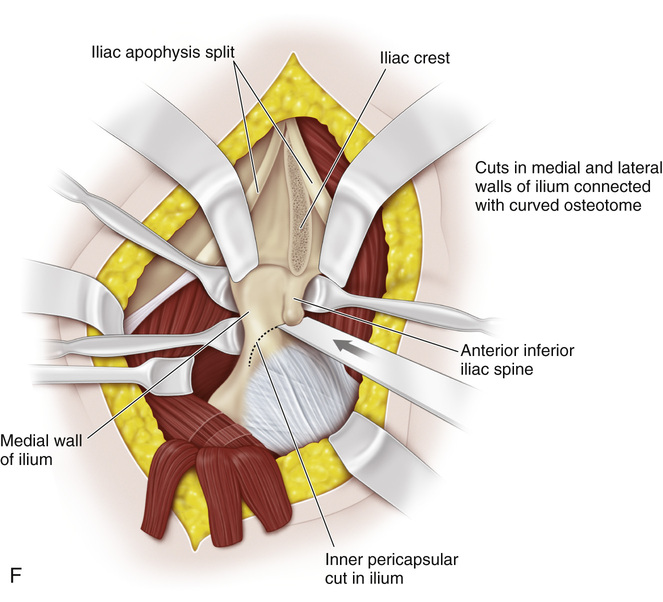
F, With sharp curved osteotomes, the cuts of the inner and outer table of the ilium are joined. Periosteal elevators are used to mobilize the osteotomized fragments, and the inferior segment of the ilium is leveled laterally, anteriorly, and distally.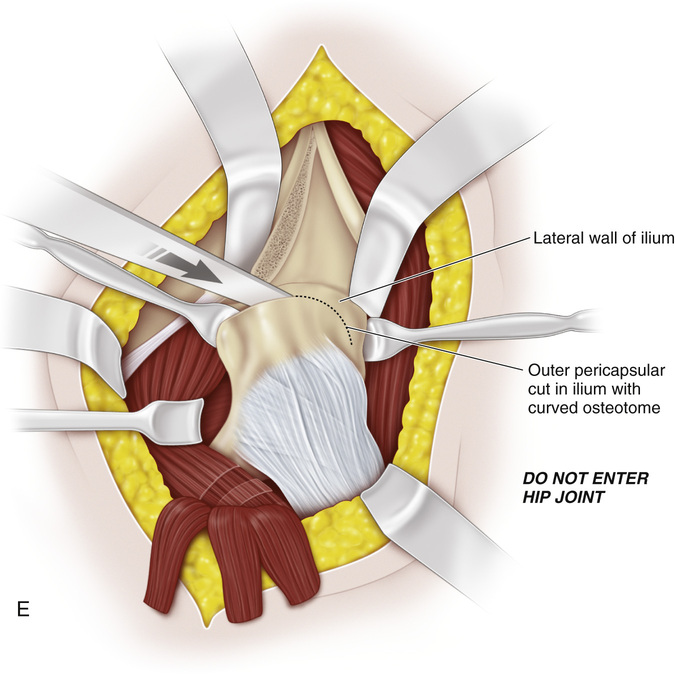
G, If necessary, a lamina spreader may be used to separate the iliac fragments. However, the operator should be very gentle; he or she should steady the upper segment of the ilium and push it distally. Care should be taken not to fracture the acetabular segment by forceful manipulation or crushing with the lamina spreader.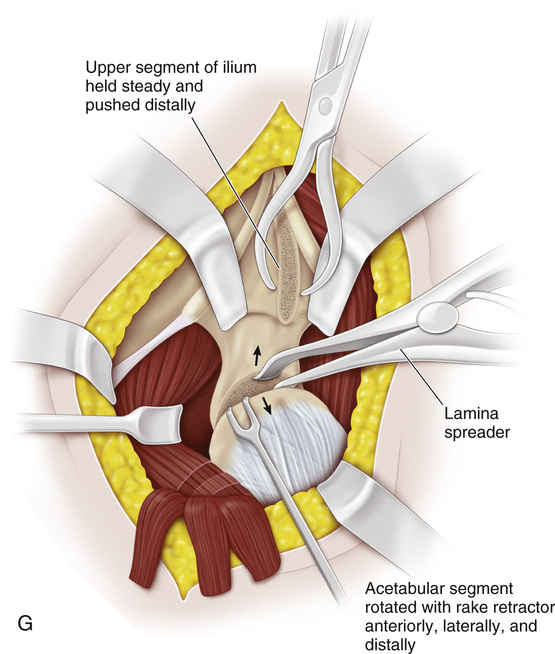
H and I, Next, a triangular wedge of bone is resected from the anterior part of the iliac wing. In the young child, we remove the wedge of bone more posteriorly and avoid the anterior superior iliac spine; this gives greater stability to the iliac fragments. The wedge of bone graft may be shaped into a curve to fit the graft site. Pemberton and Coleman recommend that grooves be made on the opposing cancellous surfaces of the osteotomy. The graft is impacted into the grooves, and the osteotomized fragment is sufficiently stable to obviate internal fixation. We do not recommend cutting grooves because of the associated problems of splintering and the weakening of the acetabulum. The fragments are fixed internally with two threaded Kirschner pins or cancellous screws. The internal fixation allows the surgeon to remove the cast sooner, to mobilize the hip, and to prevent joint stiffness. The sartorius muscle is reattached to its origin, the split iliac apophysis is sutured, and the wound is closed in the usual fashion. A one-and-one-half-hip spica cast is applied.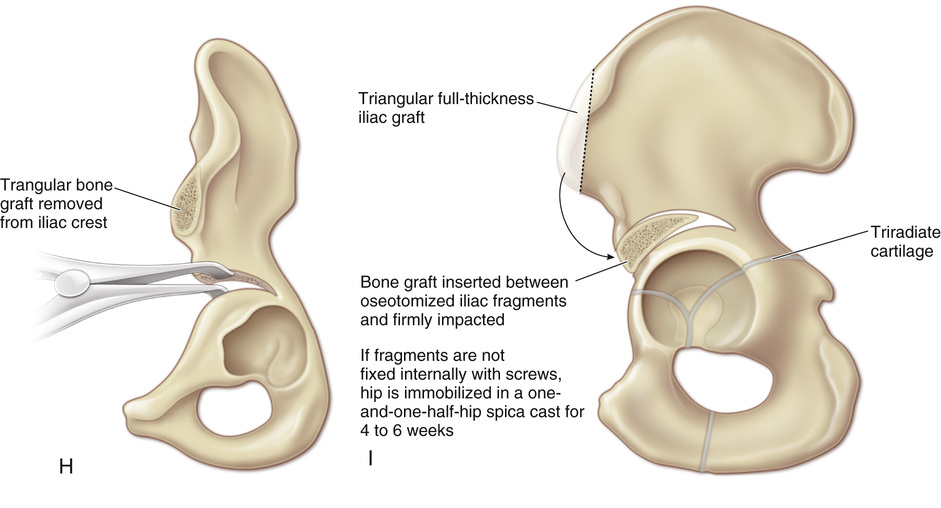
Related posts:
 23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
33 Triple Arthrodesis
58 Arthrodesis of the Ankle Joint via the Anterior Approach Without Disturbing the Distal Tibial Growth Plate
12 Ganz Periacetabular Osteotomy
23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
33 Triple Arthrodesis
58 Arthrodesis of the Ankle Joint via the Anterior Approach Without Disturbing the Distal Tibial Growth Plate
12 Ganz Periacetabular Osteotomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


