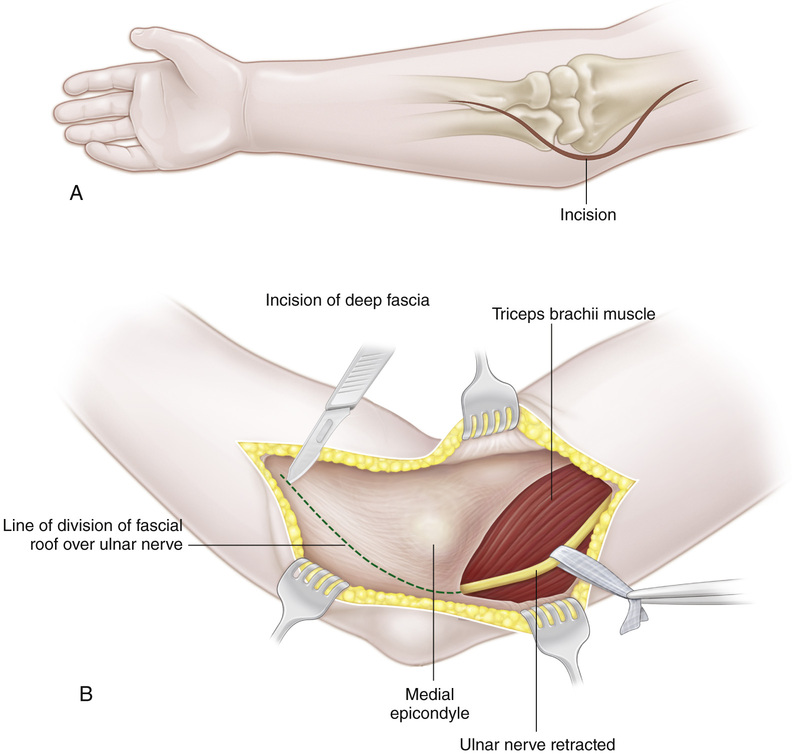
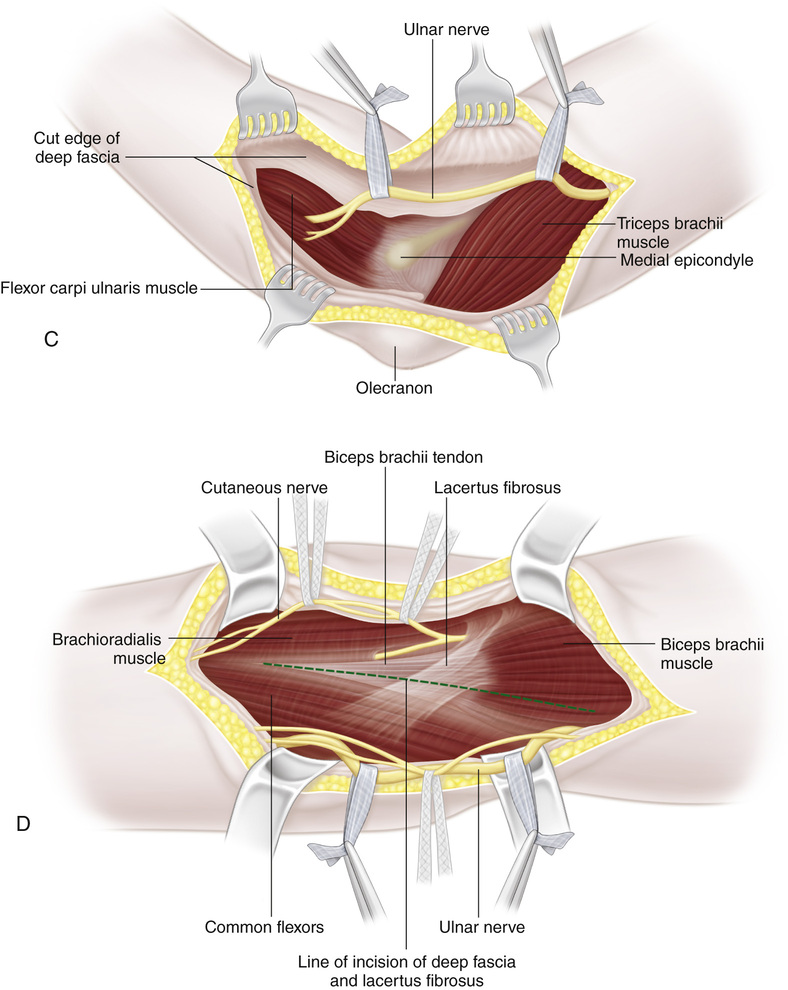
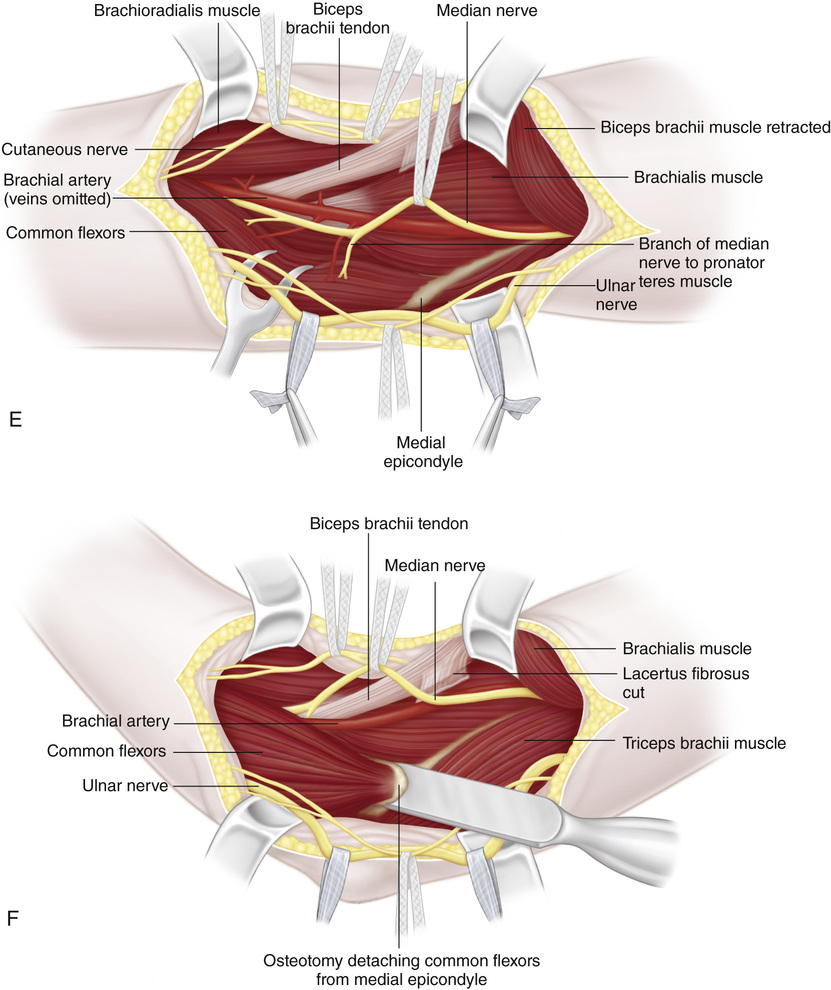
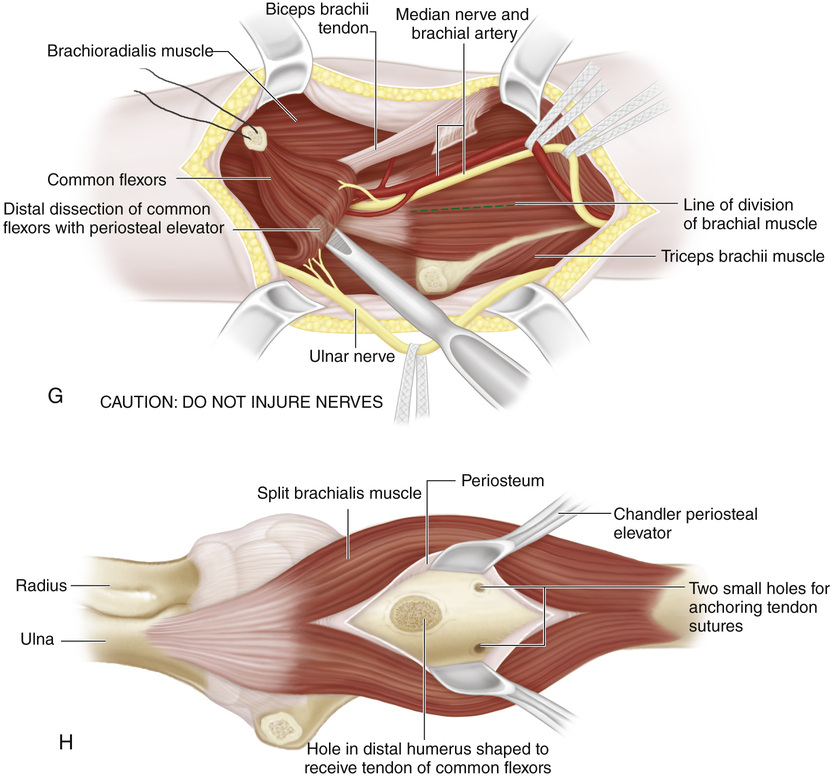
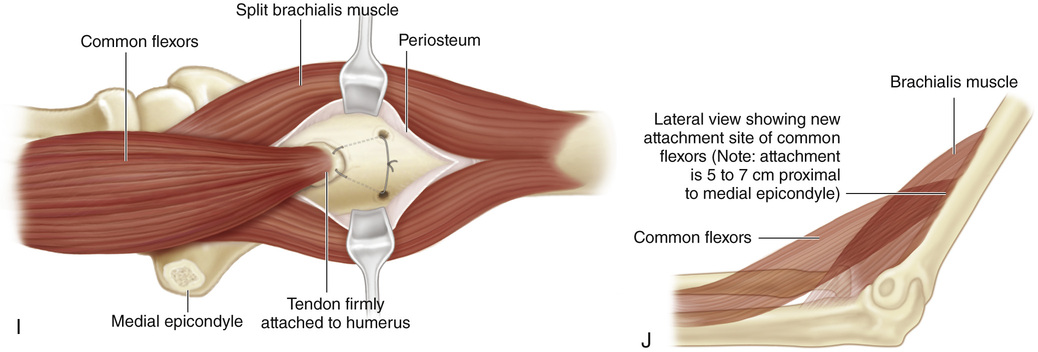
A, With the elbow in extension, a curved longitudinal incision is made over the anteromedial side of the elbow, beginning approximately 3 in above the flexion crease of the elbow joint over the medial intermuscular septum and extending distally to the anterior aspect of the medial epicondyle. At the joint level it turns anterolaterally on the volar surface of the forearm along the course of the pronator teres muscle for a distance of approximately 2 in. B, The subcutaneous tissue and fascia are divided in line with the skin incision, and the skin flaps are widely mobilized and retracted. Next the ulnar nerve is located posterior to the medial intermuscular septum and lying in a groove on the triceps muscle. It is isolated, and moist hernia tape is passed around it for gentle handling. The ulnar nerve is traced distally to its groove between the posterior aspect of the medial epicondyle of the humerus and the olecranon process. The fascial roof over the ulnar nerve is carefully divided under direct vision over a grooved director. C, The ulnar nerve is dissected free distally to the point where it passes between the two heads of the flexor carpi ulnaris muscle. Inadvertent damage to branches of the ulnar nerve to the flexor carpi ulnaris should be avoided. A second piece of hernia tape is passed around the ulnar nerve in the distal part of the wound, and the nerve is retracted posteriorly. D, Next the biceps tendon is identified over the anterior aspect of the elbow joint. The deep fascia and the lacertus fibrosus are divided along the medial aspect of the biceps tendon. E, By digital palpation, the interval between the biceps and pronator teres muscle is developed. The brachial artery with its accompanying veins runs along the medial side of the biceps tendon. The median nerve, lying medial to the brachial artery, is dissected free of surrounding tissue and gently retracted anteriorly with moist hernia tape. The branches of the median nerve to the pronator teres muscle must be identified and protected from injury. F, Next, with an osteotome, the common flexor origin of the pronator teres, the flexor carpi radialis, the palmaris longus, the flexor digitorum sublimis, and the flexor carpi ulnaris is detached en bloc with a flake of bone from the medial epicondyle. G, By sharp and blunt dissection, the flexor muscle mass is freed and mobilized distally away from the joint capsule and the ulna as far as the motor branches of the median nerve and ulnar nerve will permit. A no. 1 silk whip suture is placed in the proximal end of the common flexors. H, The biceps muscle, brachial vessels, and median nerve are retracted laterally, and the atrophied brachial muscle is split longitudinally. The periosteum is incised and stripped to expose the anterior aspect of the distal end of the humerus. The elbow is then flexed to 120 degrees to determine the site of attachment of the transfer (usually 2 in proximal to the elbow). With a drill, a hole is made on the anterior surface of the humerus. The opening is enlarged with progressively larger diamond-head hand drills to receive the transferred muscle. The action of the transfer as a pronator of the forearm is decreased by transferring it laterally on the humerus. With smaller drill points, two tunnels are made from the lateral and medial cortices of the humerus and connected to the larger hole for passing the suture. I and J, Because the elbow will be immobilized in acute flexion, it is best to close the distal half of the wound before anchoring the transplant to the humerus. The ends of the whip suture are brought out through the tunnels, and the common flexors and the origin are firmly secured in the larger hole. The periosteum is closed with interrupted sutures over the transferred tendon, thus reinforcing its anchorage. The proximal half of the wound is closed, and a long-arm cast is applied with the elbow in acute flexion and the forearm in full supination. For postoperative care, see the guidelines outlined in the text on principles of tendon transfer.
Flexorplasty of the Elbow (the Mayer and Green Modification of the Steindler Technique)
Operative Technique
Related posts:
 23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


