Posterior Approach for Forequarter Amputation (Littlewood Technique)
The patient is placed in the lateral position, and the neck, chest, and whole upper limb are prepared and draped. Blood loss is minimal, but adequate whole blood should be available for transfusion if necessary.
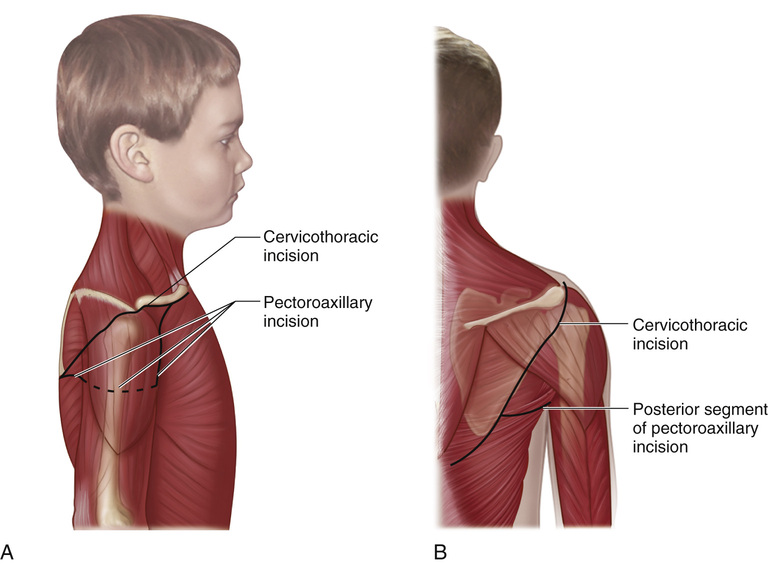
A to C, The cervicothoracic incision begins at the medial end of the clavicle and extends laterally along the anteroinferior border of the clavicle to the lateral protuberance of the acromion, where it curves posteriorly. It is then continued along the lateral border of the scapula to its inferior angle, where it curves medially to terminate 3 to 4 cm lateral to the midline of the spine.
The pectoroaxillary incision begins at the center of the clavicle and extends inferolaterally along the deltopectoral groove; it then crosses the anterior axillary fold and joins the posterior incision at the lower third of the lateral border of the scapula. The subcutaneous tissue and fascia are divided in line with the skin incision, and the wound flaps are mobilized to expose the underlying muscles.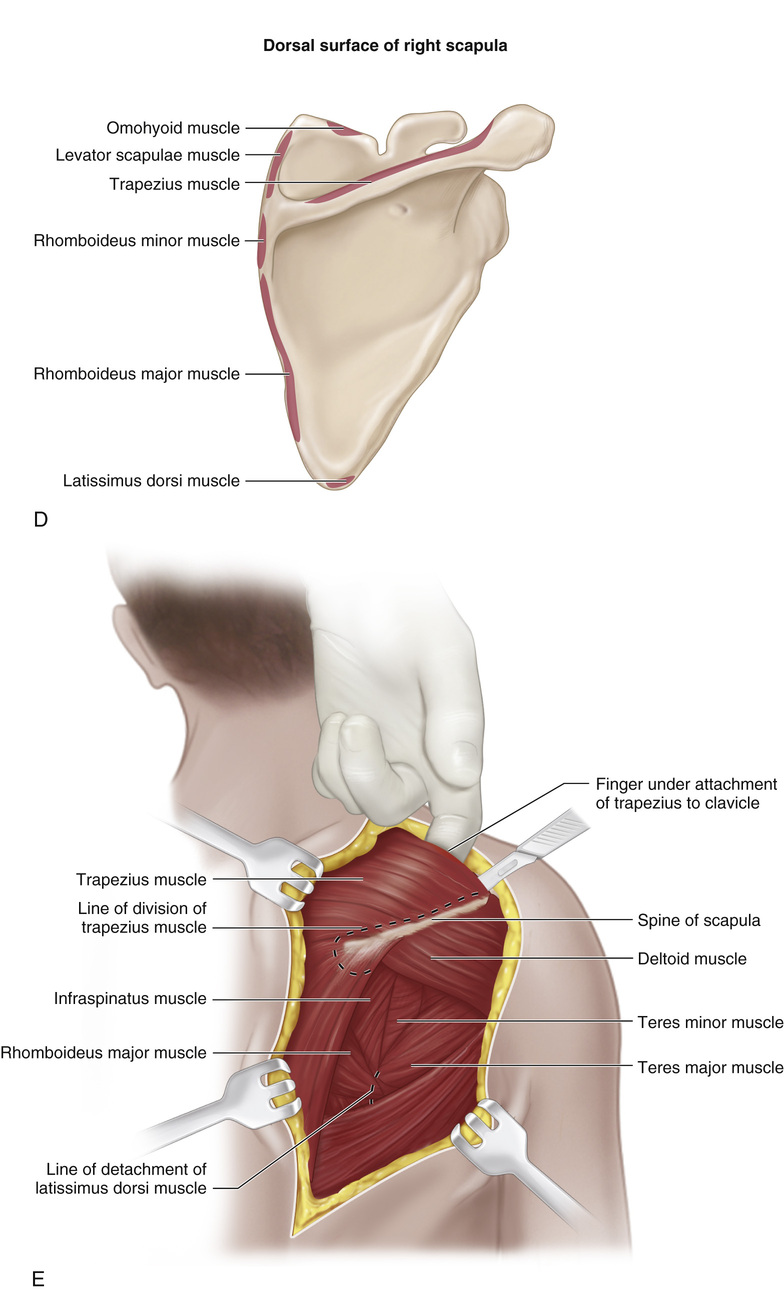
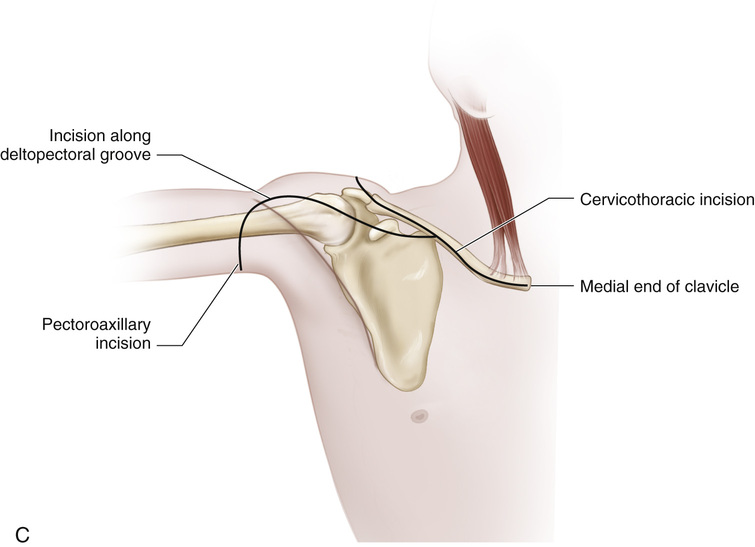
D and E, The muscles connecting the scapula to the trunk are detached from the scapula in layers and marked with silk whip sutures. First, the trapezius and latissimus dorsi are divided.
F, Next, the omohyoid, levator scapulae, and rhomboid muscles are detached. Transverse cervical and transverse scapular vessels are ligated and divided as dissection proceeds. The cords of the brachial plexus are sectioned with a very sharp scalpel near their origin.
G and H, The scapula is retracted forward, and the serratus anterior muscle is sectioned and detached from the scapula.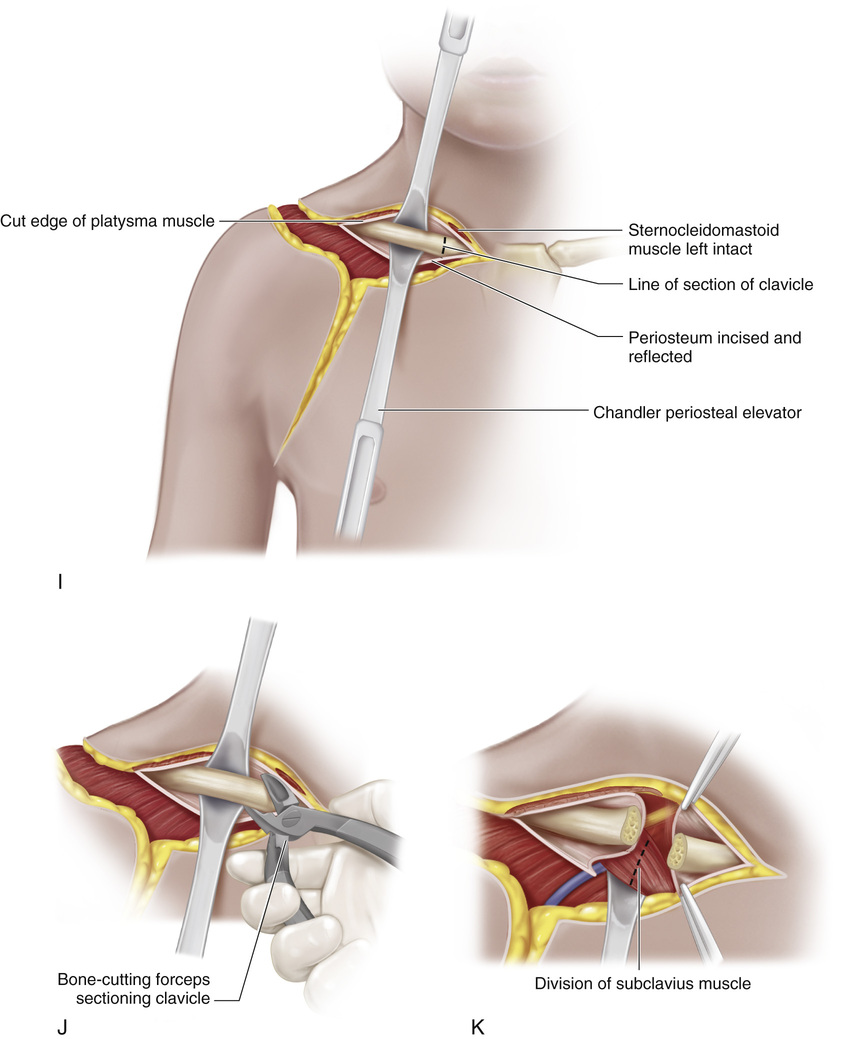
I to K, The patient is turned onto her or his back, and the medial end of the clavicle is exposed subperiosteally. Lever-type retractors are placed deep to the clavicle to protect the underlying neurovascular structures. With bone-cutting forceps or a Gigli saw, the clavicle is sectioned near its sternal attachment. The subclavius muscle is divided next.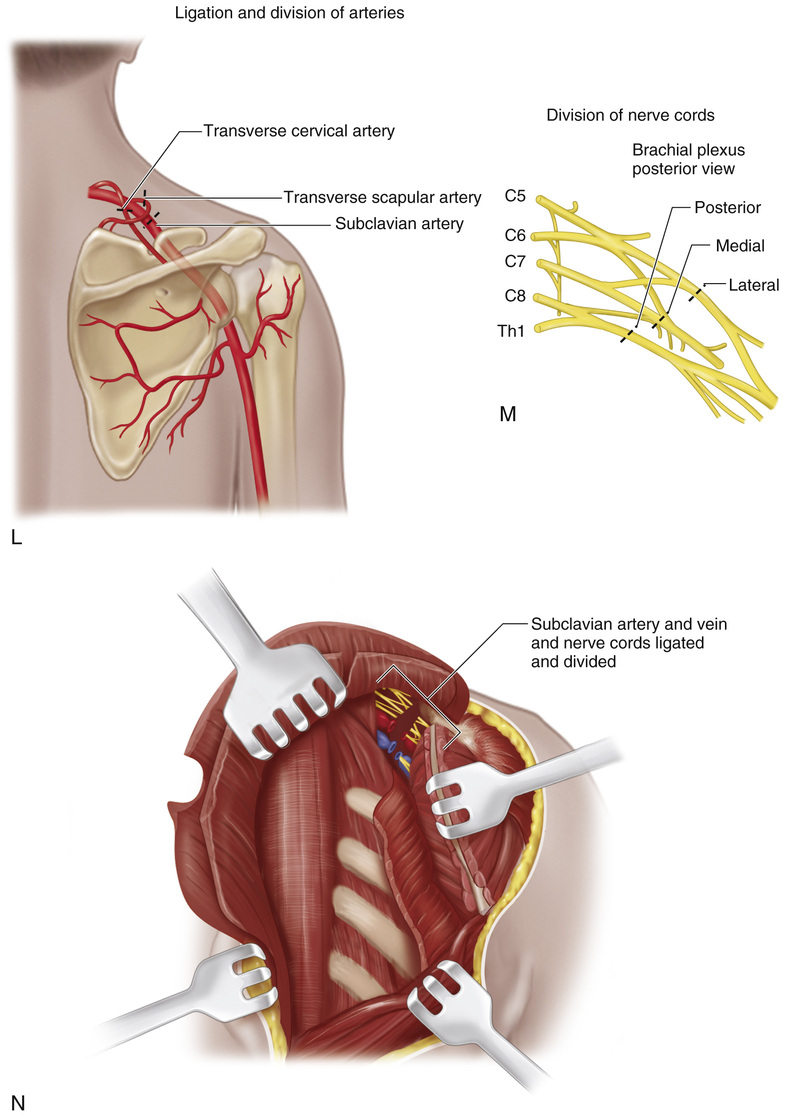
L to N, The subclavian vessels and brachial plexus are exposed by allowing the upper limb to fall anteriorly. The subclavian artery and vein are isolated, individually clamped, doubly ligated with sutures, and divided.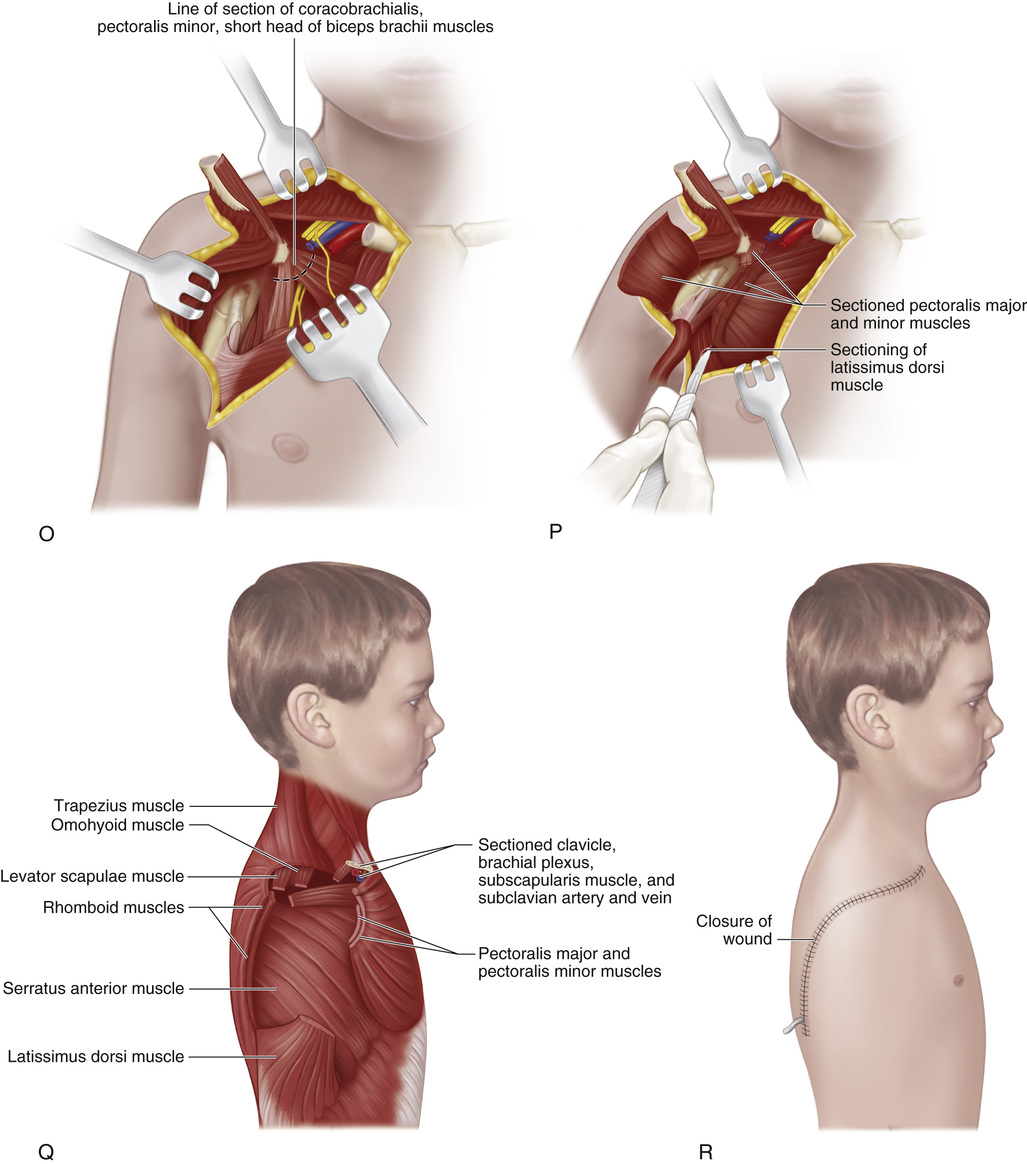
O to Q, The pectoralis major and minor, short head of the biceps, coracobrachialis, and latissimus dorsi are sectioned, completing ablation of the limb.
R, The wound flaps are approximated and sutured together. Closed suction catheters are inserted and connected to an evacuator. A firm compression dressing is applied.
Related posts:
 23 Hamstring Lengthening
23 Hamstring Lengthening
 29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
 10 Pemberton Osteotomy
10 Pemberton Osteotomy
 33 Triple Arthrodesis
33 Triple Arthrodesis
 7 Distal and Lateral Transfer of the Greater Trochanter
7 Distal and Lateral Transfer of the Greater Trochanter
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


