Woodward Operation for Congenital High Scapula
The operation is performed with the patient in the prone position, the head supported on a craniotomy headrest, and the neck in slight flexion. The sides and back of the neck, both shoulders, the trunk down to the iliac crests, and the upper limb on the involved side are prepared and draped. One should be able to manipulate the shoulder girdle and arms during the operation without contaminating the surgical field.
Operative Technique
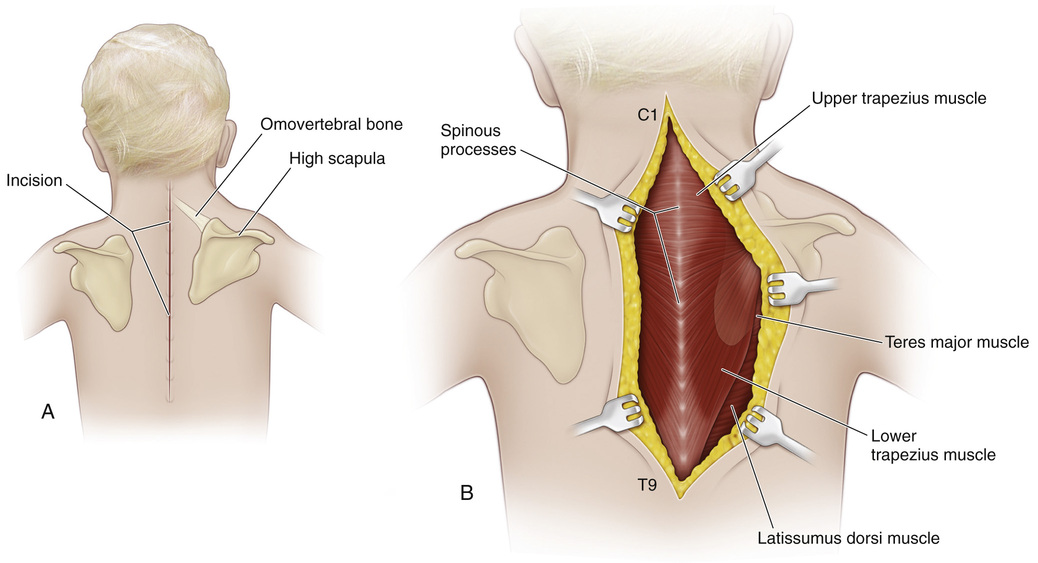
A, A midline longitudinal incision is made that extends from the spinous process of the first cervical vertebra to that of the ninth thoracic vertebra.
B, The subcutaneous tissue is divided in line with the skin incision. The wound margins are undermined laterally to the medial border of the scapula. The muscle arrangement should be clearly visualized.
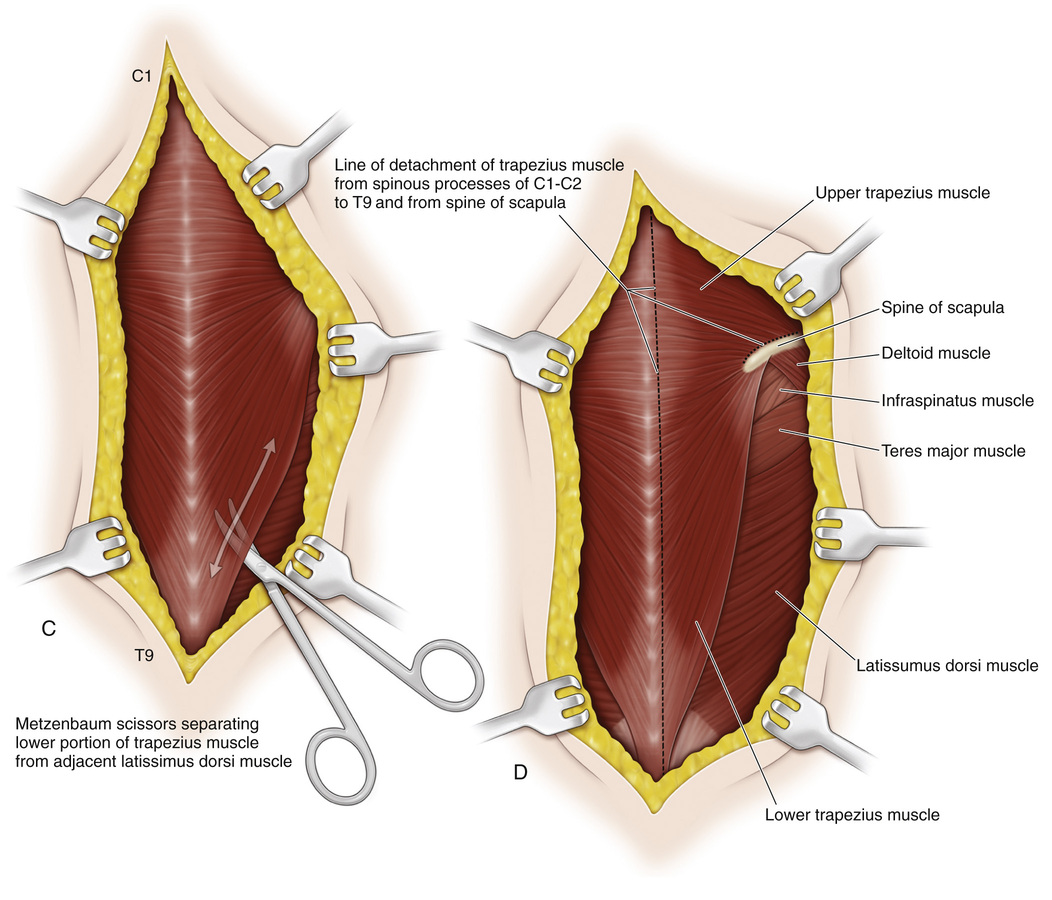
C, Next, the lateral border of the trapezius muscle is identified at the distal part of the wound. By blunt dissection, the lower portion of the trapezius is separated from the subjacent latissimus dorsi muscle.
D, With a sharp scalpel the tough and tendinous origin of the trapezius muscle is detached from the spinous process. Numerous sutures are passed at the entire origin of the muscle to mark it and for use at later reattachment.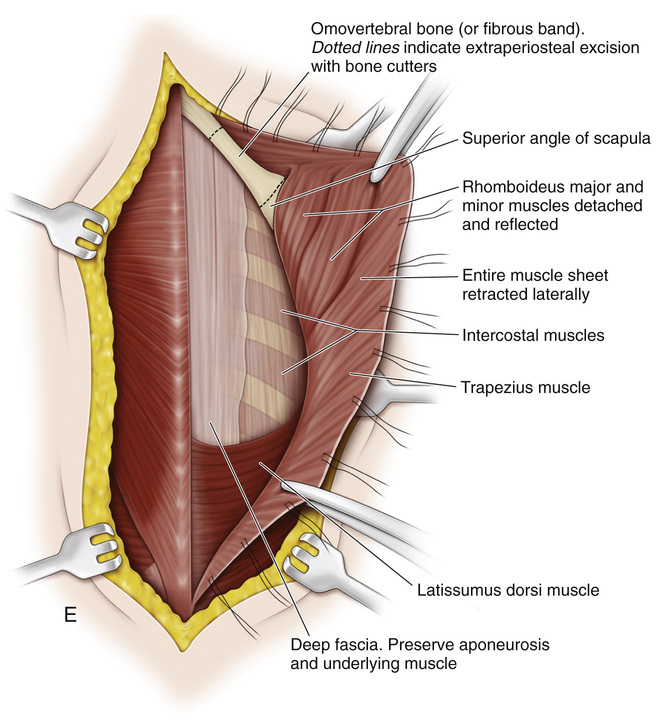
E, In the upper part of the incision the origins of the rhomboideus major and minor muscles are sharply divided and tagged with sutures. A well-defined deep layer of fascia separates the rhomboids and the upper part of the trapezius from the serratus posterior superior and erector spinae muscles. It is vital to maintain a proper tissue plane. Preserve the aponeurosis and muscle sheet intact for secure fixation of the scapula at its lowered level.
Next, the entire muscle sheet is retracted laterally to expose the omovertebral bone or fibrous band if present. The omovertebral bar is excised extraperiosteally; it usually extends from the superior angle of the scapula to the lower cervical vertebrae. It is best to use a bone cutter for resection. Avoid injury to the spinal accessory nerve, the nerves to the rhomboids, and the descending scapular artery. The contracted levator scapulae muscle is sectioned at its attachment to the scapula. Fibrous bands attached to the anterior surface of the scapula usually restrict its downward displacement; if present, they are sectioned. Next, the scapula is everted, and the serratus anterior muscle is detached from its insertion on the vertebral border of the scapula. A periosteal elevator is used to elevate the supraspinatus muscle extraperiosteally from the supraspinous portion of the scapula and the subscapularis muscle from the deep surface of the scapula midway between the superior and inferior angles. The supraspinous portion of the scapula is resected with its periosteum. The suprascapular vessels and nerves and the transverse scapular artery should be protected from injury. These steps are illustrated on Procedure 60, steps K and L, of the modified Green scapuloplasty.
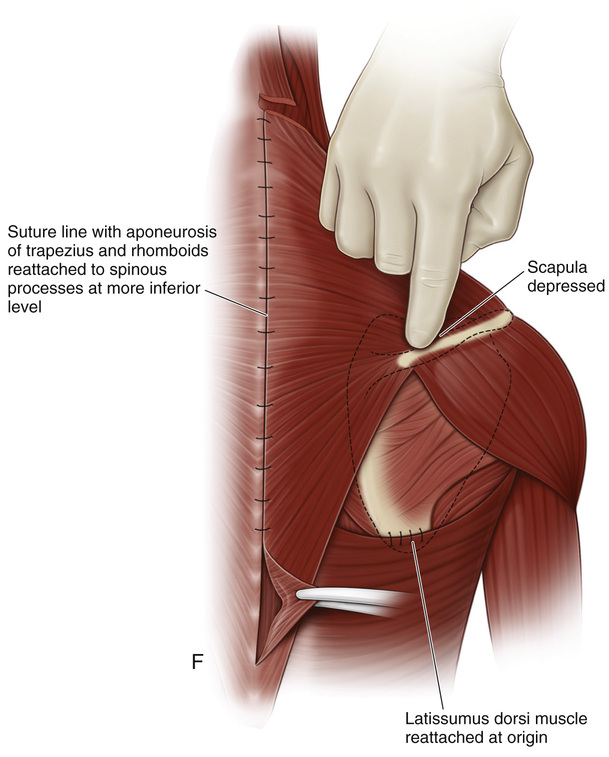
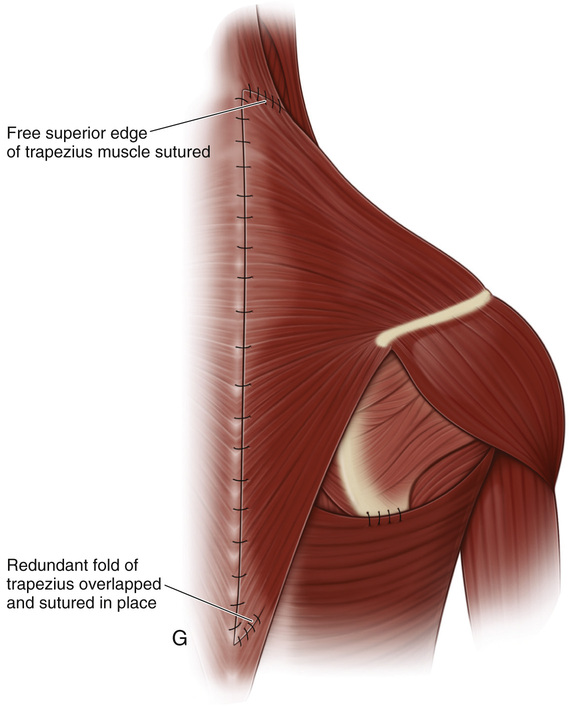
F, Next, the scapula is lowered to its normal level and held in the corrected position by an assistant. The subscapularis muscle is reattached to the vertebral border of the scapula, and the supraspinatus muscle is resutured to the scapular spine. The serratus anterior muscle is reattached to the vertebral border of the scapula at a more proximal level. The latissimus dorsi muscle is reattached to the scapula. Proceeding cephalocaudally, the thick aponeurosis of the trapezius and rhomboid muscles is sutured to the spinous processes at a more distal level. It is essential that an assistant maintain the corrected level of the scapula.
G, Because the origin of the trapezius muscle distal to the ninth thoracic vertebra is not disturbed, a redundant fold of aponeurotic tissue is created in the distal end of the trapezius muscle. This fold of soft tissue is excised and resutured.
The wound is closed in usual fashion. The skin closure is subcuticular.
Related posts:
 23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


