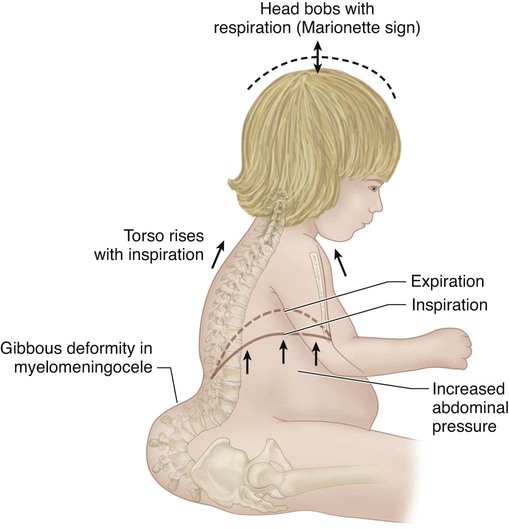
• +0: no assistance, on room air • +1: supplemental oxygen required • +2: nighttime ventilation/continuous positive airway pressure (CPAP) • +3: part time ventilation/CPAP • Normal respiratory rate at birth is 40–80 breaths per minute; that up to age 5 years, 20–40 breaths per minute; and 15–25 breaths per minutes is normal from age 6 to 12 years. Adult values, 15–20 breaths per minute, are reached after 15 years of age (Hoekelman, 1987). • Respiratory rate at rest above these values suggest occult respiratory insufficiency. • The thumb excursion test is performed to clinically measure the ability of each side of the chest to contribute to respiration by rib cage expansion. • The examiner’s hands are placed around the base of the thorax with the thumbs posteriorly pointing upward at equal distances from the spine (Fig. 1). • With respiration, the thumbs move away from the spine symmetrically because of the anterior lateral motion of the chest wall. • Each hemithorax is graded separately: • The concave fused-rib hemithorax often has a +0 thumb excursion test, and if there is significant rib hump deformity of the convex hemithorax, it will also be stiff and also have a +0 thumb excursion test. • This represents a form of secondary thoracic insufficiency syndrome in which the diaphragm, in effect, is doing a pushup against body weight because the “collapsing torso” deformities, such as lumbar kyphosis in myelomeningocele, or severe pelvic obliquity, raise abdominal pressure on the diaphragm by abnormal proximity to the pelvis (Fig. 2) (Campbell and Smith, 2007; Campbell et al., 2003b). • The AP radiograph is analyzed for Cobb’s angle, the interpedicular line ratio, the height of the thoracic spine in centimeters, and the space available for the lung. • The height of the thorax is determined by the radiographic height of the patient’s thoracic spine, and this distance is divided by the normal thoracic spinal height for age, deriving a percentage of normal. • The lateral radiograph defines a loss of sagittal depth of the thorax, due to either pectus excavatum or thoracic spinal lordosis. • The AP and lateral radiographs enable identification of the volume depletion deformities (VDDs) of the thorax in the coronal and sagittal planes of the thorax. • In type I and type II VDDs, windswept deformity of the chest is also common, with severe reduction in transverse volume of the convex hemithorax. Its severity can be defined by measurements of spinal rotation, the posterior hemithorax symmetry ratio, and the thoracic rotation of the CT “scan cut” at the level of maximum deformity. • Both ventilation-perfusion lung scans and 3-mm-cut CT scans with airway reconstruction can define airway compression deformity, if necessary. • The goal of VEPTR surgery is to brace the unstable defect with multiple VEPTRs or use VEPTRs to stabilize ribs transported into the area of defect. • Care must be taken not to damage the lung when the skin incision is over the rib cage defect, and generally there is a large spine defect in the area of the chest wall defect, so care must be taken not to violate the dura in the exposure. • The exposure should cautiously approach the defect area, first proximally, then distally. • Even if gross bony synostosis is not present, longitudinal hemithorax constriction may be present from intercostal muscle scarring, evident on supine lateral bending radiographs when the affected intercostal spaces do not widen while bending into the convex side. • A standard thoracotomy approach would place the spinal cord at risk when this abnormality is present, so the scapula should be cautiously retracted posteriorly and the rhomboid muscles sectioned directly off the edge of the scapula to avoid dural injury. • For the prone position, longitudinal soft rolls are placed under each side of the chest. • A transverse roll is placed under the pelvis. • The patient is immobilized by wide cloth tape padded with hand towels across the buttocks. • The VEPTR expansion thoracoplasty strategy for each VDD of the thorax is different. • In mixed types of VDD, VEPTR surgical treatment should address each individual segment of thoracic deformity with either appropriate longitudinal or lateral expansion of the constricted thorax. • The most common VDD of the thorax is unilateral constriction of the thorax in fused ribs and scoliosis. • The two Freer elevators should touch in the “chopstick” maneuver, to confirm that a continuous soft tissue tunnel has been made.
Vertical Expandable Prosthetic Titanium Rib (VEPTR) Expansion Thoracoplasty
Examination/Imaging
History
 A detailed surgical and respiratory history should be obtained in children with thoracic insufficiency syndrome.
A detailed surgical and respiratory history should be obtained in children with thoracic insufficiency syndrome.
Physical Examination
 The child’s ability to respond to pulmonary challenge, such as play activities and running, should be noted. Difficulty in such activities can be a helpful early warning of impending respiratory insufficiency/thoracic insufficiency.
The child’s ability to respond to pulmonary challenge, such as play activities and running, should be noted. Difficulty in such activities can be a helpful early warning of impending respiratory insufficiency/thoracic insufficiency.
 If the patient is on oxygen, or dependent on more invasive respiratory support, the degree of respiratory insufficiency should be defined by the assisted ventilator ratings (AVRs) (Campbell and Smith, 2007):
If the patient is on oxygen, or dependent on more invasive respiratory support, the degree of respiratory insufficiency should be defined by the assisted ventilator ratings (AVRs) (Campbell and Smith, 2007):
 The chest is assessed for clinical deformity and the circumference measured at the nipple line and compared to normal values for age to discern percentile of normal (Jones, 1988).
The chest is assessed for clinical deformity and the circumference measured at the nipple line and compared to normal values for age to discern percentile of normal (Jones, 1988).
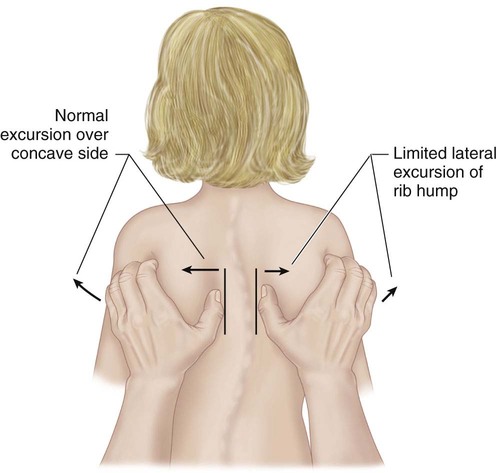
 Greater than 1 cm of excursion of each thumb away from the spine during inspiration is graded as +3, and considered normal.
Greater than 1 cm of excursion of each thumb away from the spine during inspiration is graded as +3, and considered normal.
 0.5–1 cm of excursion is graded +2.
0.5–1 cm of excursion is graded +2.
 Motion up to 0.5 cm is graded as +1.
Motion up to 0.5 cm is graded as +1.
 Assess for a marionette sign: the patient’s head bobs synchronously with respiration.
Assess for a marionette sign: the patient’s head bobs synchronously with respiration.
Imaging Studies
 Weight-bearing anteroposterior (AP) and lateral radiographs of the entire spine, including the chest and pelvis on the same radiograph, are obtained.
Weight-bearing anteroposterior (AP) and lateral radiographs of the entire spine, including the chest and pelvis on the same radiograph, are obtained.
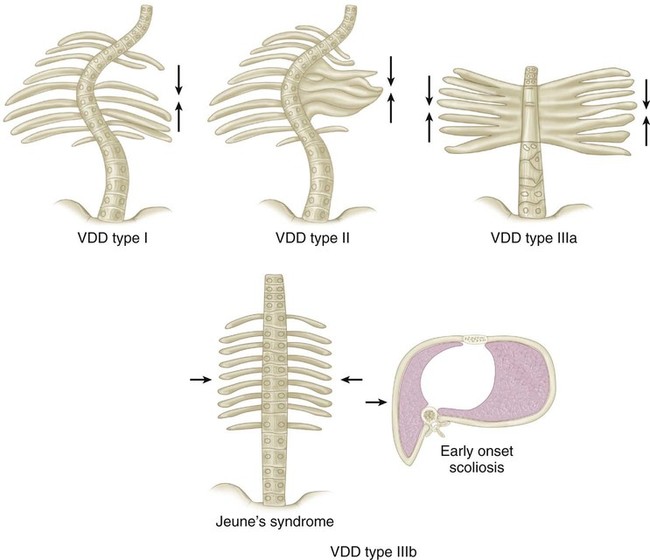
 Computed tomography (CT) scans of the entire chest and lumbar spine are performed at 5-mm intervals, unenhanced, with the scanner set for pediatric dosage to minimize radiation exposure (Campbell and Hell-Vocke, 2003; DiMeglio and Bonnel, 1990; Gollogly et al., 2004a; Gollogly et al., 2004b; Paterson et al., 2001). Usually type I, type II, and type III VDDs have a diminished thoracic volume on CT scan in the coronal plane reconstructions (Fig. 3) (Openshaw et al., 1984).
Computed tomography (CT) scans of the entire chest and lumbar spine are performed at 5-mm intervals, unenhanced, with the scanner set for pediatric dosage to minimize radiation exposure (Campbell and Hell-Vocke, 2003; DiMeglio and Bonnel, 1990; Gollogly et al., 2004a; Gollogly et al., 2004b; Paterson et al., 2001). Usually type I, type II, and type III VDDs have a diminished thoracic volume on CT scan in the coronal plane reconstructions (Fig. 3) (Openshaw et al., 1984).
 CT lung scan volumes can be computed. Full-chest CT scans may be taken at yearly follow-up if percent normal lung volumes are being followed to detect progressive thoracic volume loss.
CT lung scan volumes can be computed. Full-chest CT scans may be taken at yearly follow-up if percent normal lung volumes are being followed to detect progressive thoracic volume loss.
 Either ultrasound or fluoroscopy of the diaphragm can be performed to document diaphragmatic function, but dynamic MRI study of the lungs will show great detail of diaphragm and chest wall function (Campbell et al., 2008a).
Either ultrasound or fluoroscopy of the diaphragm can be performed to document diaphragmatic function, but dynamic MRI study of the lungs will show great detail of diaphragm and chest wall function (Campbell et al., 2008a).
Surgical Anatomy
 Instability of the chest wall is documented on radiographs and CT scans, and degree of paradoxical chest wall motion over the bony defect is confirmed on physical examination (Campbell and Smith, 2003).
Instability of the chest wall is documented on radiographs and CT scans, and degree of paradoxical chest wall motion over the bony defect is confirmed on physical examination (Campbell and Smith, 2003).
 Stable rib attachment sites for device placement are evaluated on radiographs.
Stable rib attachment sites for device placement are evaluated on radiographs.
Positioning
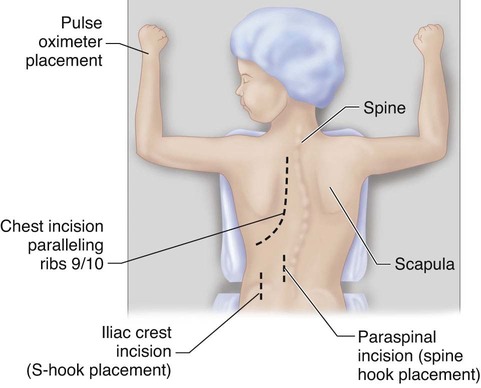
 The prone position is now most commonly used (Fig. 4).
The prone position is now most commonly used (Fig. 4).
Portals/Exposures
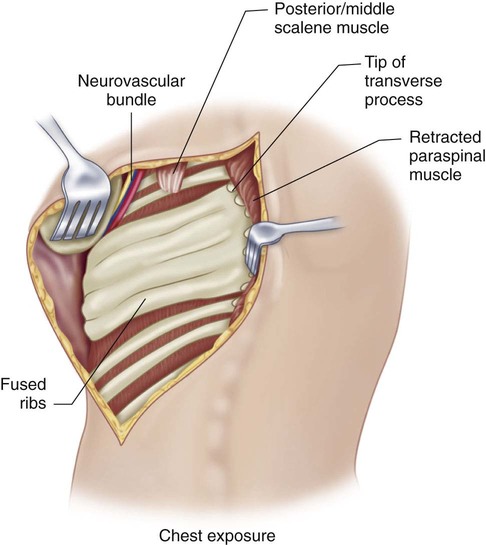
 A modified curvilinear thoracotomy incision is used, extending anteriorly between the ninth and tenth ribs.
A modified curvilinear thoracotomy incision is used, extending anteriorly between the ninth and tenth ribs.
 The trapezius, latissimus, and rhomboid muscles are sectioned in line with the skin incision.
The trapezius, latissimus, and rhomboid muscles are sectioned in line with the skin incision.
 Care must be taken not to excessively expose the spine in order to prevent inadvertent fusion.
Care must be taken not to excessively expose the spine in order to prevent inadvertent fusion.
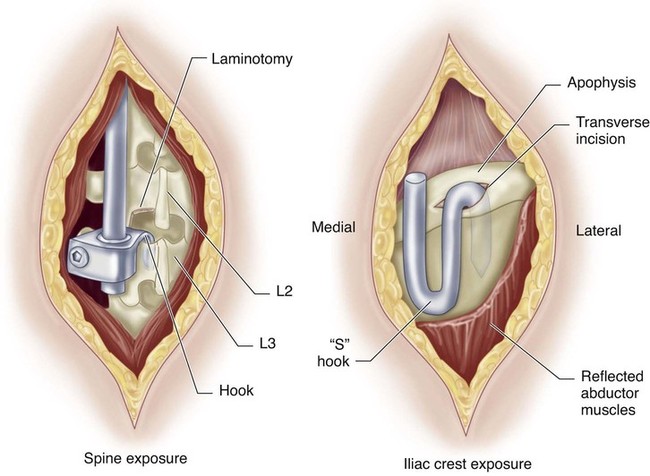
 If a distal attachment for a hybrid device is needed, a separate longitudinal paraspinous skin incision, 5 cm long, is then made 1 cm lateral to the midline at the level of the proximal lumbar spine (Fig. 5).
If a distal attachment for a hybrid device is needed, a separate longitudinal paraspinous skin incision, 5 cm long, is then made 1 cm lateral to the midline at the level of the proximal lumbar spine (Fig. 5).
 The ligamentum flavum is then resected. Gel foam is placed over the exposed dura.
The ligamentum flavum is then resected. Gel foam is placed over the exposed dura.
 If posterior elements are lacking, an S-hook over the central iliac crest may be used for hybrid attachment (Fig. 6).
If posterior elements are lacking, an S-hook over the central iliac crest may be used for hybrid attachment (Fig. 6).
VEPTR Expansion Thoracoplasty
 VEPTR expansion thoracoplasty is a general category of surgical procedures that can expand the volume-constricted thorax when there is three-dimensional deformity of the thorax due to spine deformity, as well as primary rib cage deformity.
VEPTR expansion thoracoplasty is a general category of surgical procedures that can expand the volume-constricted thorax when there is three-dimensional deformity of the thorax due to spine deformity, as well as primary rib cage deformity.
 Multiple types of expansion thoracoplasties address each type of VDD of the thorax.
Multiple types of expansion thoracoplasties address each type of VDD of the thorax.
 The VEPTR device is made by Synthes Spine Company of West Chester, PA, and is available as a Humanitarian Use Device under an FDA Humanitarian Device Exemption, with Institutional Review Board approval required for the use of the device at each institution.
The VEPTR device is made by Synthes Spine Company of West Chester, PA, and is available as a Humanitarian Use Device under an FDA Humanitarian Device Exemption, with Institutional Review Board approval required for the use of the device at each institution.
Procedure: VDD Type II, Fused Ribs and Scoliosis
Step 1
 The VEPTR expansion thoracoplasty for this VDD is an opening wedge thoracostomy.
The VEPTR expansion thoracoplasty for this VDD is an opening wedge thoracostomy.
Related posts:
 4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
32: Patellar Instability: Lateral Release and Medial Plication
31: Discoid Lateral Meniscus
39: Open Reduction and Internal Fixation of Tibial Tubercle Fractures
59: Posterior Instrumented Reduction and Fusion for Spondylolisthesis
4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
32: Patellar Instability: Lateral Release and Medial Plication
31: Discoid Lateral Meniscus
39: Open Reduction and Internal Fixation of Tibial Tubercle Fractures
59: Posterior Instrumented Reduction and Fusion for Spondylolisthesis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


54: Vertical Expandable Prosthetic Titanium Rib (VEPTR) Expansion Thoracoplasty




































