Split Transfer of the Tibialis Anterior Tendon
Examination/Imaging
 The peroneus longus may be relatively weaker, allowing the tibialis anterior to “over-pull” the midfoot into supination and cavus, especially during early stance and during the swing phase of gait.
The peroneus longus may be relatively weaker, allowing the tibialis anterior to “over-pull” the midfoot into supination and cavus, especially during early stance and during the swing phase of gait.
 The gastrocnemius-soleus and tibialis posterior must also be assessed for contracture.
The gastrocnemius-soleus and tibialis posterior must also be assessed for contracture.
 The goal is a balanced foot in both stance and gait.
The goal is a balanced foot in both stance and gait.
 Hindfoot varus flexibility may be tested with the Coleman block test (Coleman and Chestnut, 1977).
Hindfoot varus flexibility may be tested with the Coleman block test (Coleman and Chestnut, 1977).
Portals/Exposures
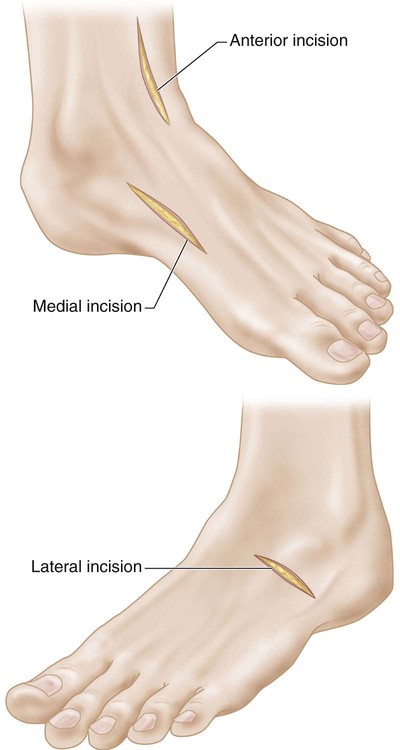
 Three incisions are outlined in Figure 1:
Three incisions are outlined in Figure 1:
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 28: Femur Fracture: Closed Reduction and Spica Cast
28: Femur Fracture: Closed Reduction and Spica Cast
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


52: Split Transfer of the Tibialis Anterior Tendon









