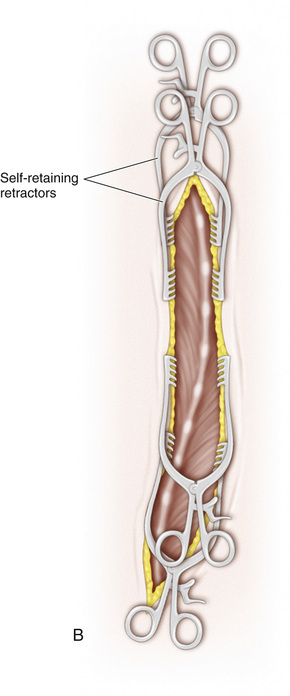
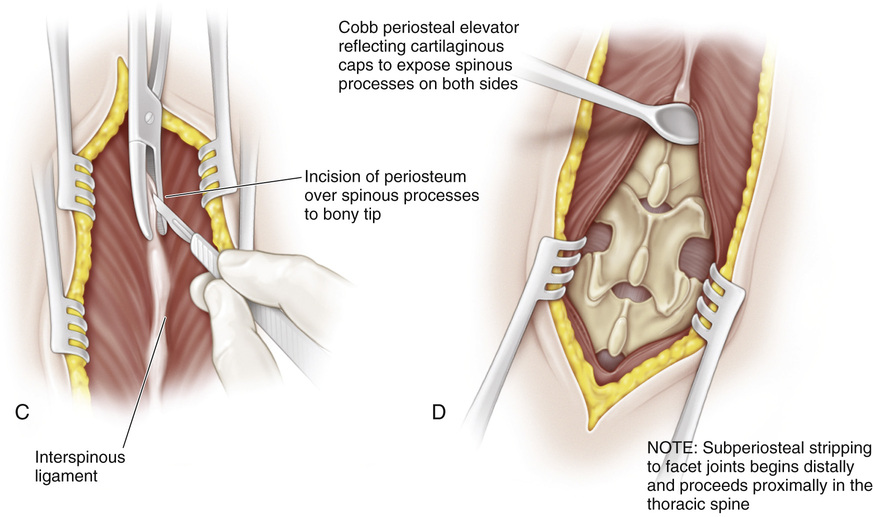
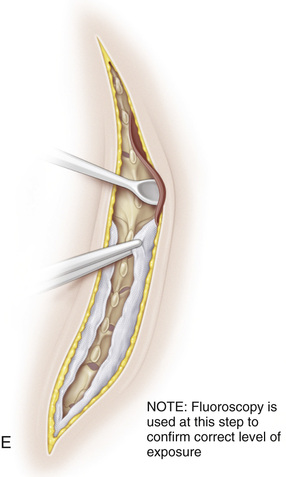
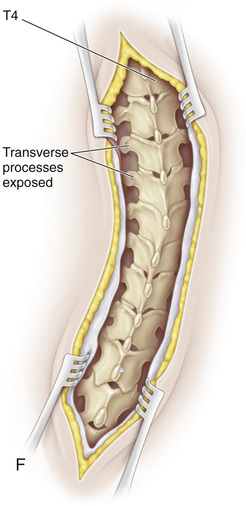
General anesthesia is administered via endotracheal intubation. Intravenous access is obtained, followed by placement of a radial arterial line. Perioperative antibiotics, usually first-generation cephalosporins, are administered. A, Positioning the patient. Under the supervision of the surgeon, the patient is placed prone on an OSI frame. Gel pads may be placed over the four support pads to further cushion the chest and inguinal region. The abdomen is free of any contact to minimize blood loss. The upper pads rest on the upper part of the chest just lateral to the nipple region. The shoulders are abducted and the elbows are flexed. The axillae should be free of pressure, without stretching across the brachial plexus or pressure over the ulnar nerve (at the elbow). The lower pads make contact at the ilioinguinal region. Unless the lateral femoral cutaneous nerve is padded satisfactorily, pressure can lead to temporary postoperative dysesthesia in the anterior aspect of the thigh. When instrumented into the lumbar spine, the hips should be extended by elevating the legs with pillows placed under the anterior part of the thigh to ensure that lumbar lordosis is maintained. The entire back is prepared with povidone-iodine (Betadine) or chlorhexidine, beginning at the base of the hairline and continuing to the gluteal cleft. Both iliac crests are included in the surgical field. After preparation and draping, a Betadine-impregnated, sticky drape is applied. An adequate area must be exposed so that the incision never extends to the edge of the drapes. B, Incision. The length of the skin incision is determined by the number of levels requiring fusion. The incision is taken down to the dermis with a scalpel. To minimize bleeding, electrocautery is used to continue the incision down through the dermis into subcutaneous tissue. An alternative to this technique is to infiltrate the intradermal tissue with epinephrine and then sharply incise down to the subcutaneous tissue. Self-retaining retractors are next placed into the wound to keep the skin edges under tension and provide exposure of the spinous processes. (Although minimally invasive surgery has been attempted for adolescent idiopathic scoliosis, the results have not been widely reported and it probably does not have any significant advantages. Early reports suggest longer surgery and little benefit with respect to shorter hospital stays, and it is far too early to determine the incidence of pseudarthrosis, a significant risk given the limited exposure.) C, Once the spinous processes have been exposed, the median raphe is incised sharply down to bone. A Kelly clamp may provide proper orientation for the incision. Dissection in this avascular plane minimizes blood loss. D, Cobb elevators are used to subperiosteally expose the posterior elements. The exposure extends laterally to the tips of the transverse processes of all the levels included in the fusion. Meticulous dissection should be performed to prepare the posterior elements for fusion. E, As the subperiosteal dissection continues, each level is packed firmly with gauze to minimize bleeding. F, Once the dissection is completed, the packing is removed and self-retaining retractors are placed at the proximal, distal, and intermediate areas. Further cleaning of the surgical field is then performed with rongeurs, curets, and electrocautery. Intraoperative fluoroscopy is used to confirm the proper levels for fusion. Regardless of the surgeon’s expertise, fluoroscopy should always be performed to avoid inadvertent selection of the wrong vertebral level. After exposure of the surgical field, anchor sites (hooks, wires, or screws) are prepared. Preoperative planning for proper hook and screw placement should be noted on the radiograph and should be familiar to all those assisting in the operation.
Exposure of the Spine for Posterior Instrumentation and Fusion
Operative Technique

Related posts:
 23 Hamstring Lengthening
23 Hamstring Lengthening
 29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
 10 Pemberton Osteotomy
10 Pemberton Osteotomy
 33 Triple Arthrodesis
33 Triple Arthrodesis
 7 Distal and Lateral Transfer of the Greater Trochanter
7 Distal and Lateral Transfer of the Greater Trochanter
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


