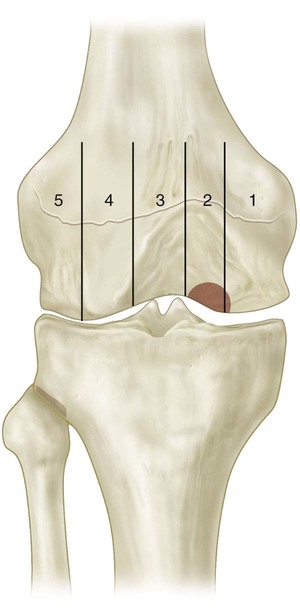
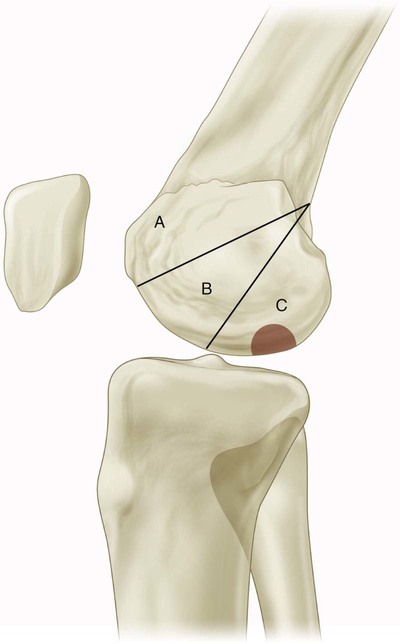
• Radiographic grading (Berndt and Harty)—anteroposterior, lateral, sunrise, and notch views • Bone scan grading (Cahill and Berg) useful for determining healing potential • MRI staging (Hefti et al.) (Figs. 1–3) • Arthroscopic grading (Ewing and Voto/International Cartilage Repair Society) Treatment Options Three-Phase Nonoperative Management Protocol (Flynn and Kocher, 2004) • Posterolateral medial femoral condyle—70% (often only seen on notch view) (Figs. 4 and 5) • Inferocentral lateral femoral condyle—20%
Osteochondritis Dissecans Fixation
Examination/Imaging
 The patient often reports aching, activity-related anterior knee pain. The presentation can be quite similar to patellofemoral syndrome. The presence of OCD should be considered when making the diagnosis of patellofemoral stress syndrome.
The patient often reports aching, activity-related anterior knee pain. The presentation can be quite similar to patellofemoral syndrome. The presence of OCD should be considered when making the diagnosis of patellofemoral stress syndrome.
 Other findings on physical examination include an antalgic gait.
Other findings on physical examination include an antalgic gait.
 I—visible on radiograph, normal bone scan
I—visible on radiograph, normal bone scan
 II—increased uptake in lesion only
II—increased uptake in lesion only
 III—increased uptake in lesion + femoral condyle
III—increased uptake in lesion + femoral condyle
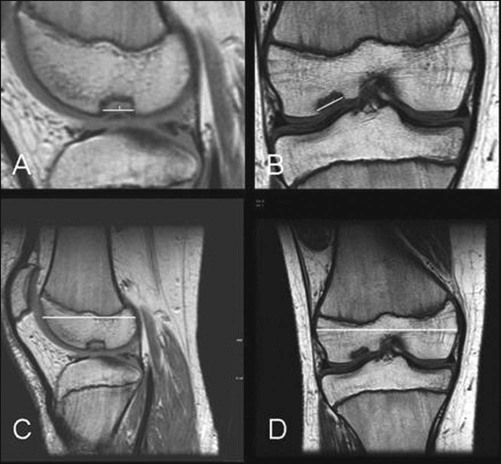

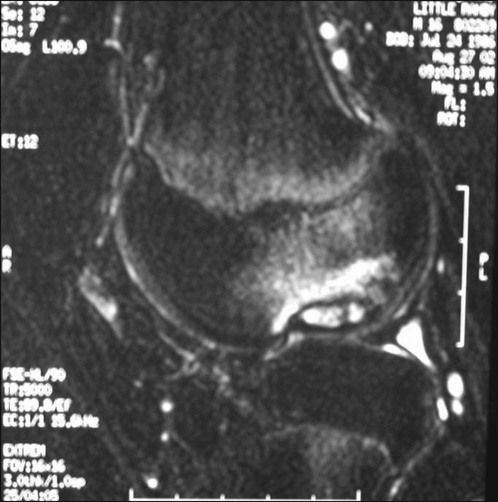
 Stage I—small signal change, no clear margins
Stage I—small signal change, no clear margins
 Stage II—fragment with clear margins without fluid between fragment and bone
Stage II—fragment with clear margins without fluid between fragment and bone
 Stage III—fluid partially visible between fragment and bone
Stage III—fluid partially visible between fragment and bone
 Stage IV—fluid completely surrounds fragment
Stage IV—fluid completely surrounds fragment
Surgical Anatomy
 It is important to perform a complete arthroscopic survey of the knee when evaluating OCD. Fissuring of the chondral surface can lead to loose bodies. These loose bodies should be removed at the time of the operation (Fig. 6)
It is important to perform a complete arthroscopic survey of the knee when evaluating OCD. Fissuring of the chondral surface can lead to loose bodies. These loose bodies should be removed at the time of the operation (Fig. 6)Related posts:
 4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
32: Patellar Instability: Lateral Release and Medial Plication
31: Discoid Lateral Meniscus
39: Open Reduction and Internal Fixation of Tibial Tubercle Fractures
59: Posterior Instrumented Reduction and Fusion for Spondylolisthesis
4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
32: Patellar Instability: Lateral Release and Medial Plication
31: Discoid Lateral Meniscus
39: Open Reduction and Internal Fixation of Tibial Tubercle Fractures
59: Posterior Instrumented Reduction and Fusion for Spondylolisthesis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


36: Osteochondritis Dissecans Fixation




























