PROCEDURE 33 Knee Surgery for Children with Cerebral Palsy I: Hamstring Lengthening Benjamin J. Shore and Brian Snyder • As a child with cerebral palsy matures, incongruous growth between the muscle and bone occurs so that the muscle is relatively shorter than the bone it subtends. Biarticular muscles tend to be more affected than monoarticular muscles; this pattern appears to be more profound distally than proximally, resulting in contractures of the gastrocnemius-soleus, hamstrings, rectus femoris, and psoas muscles. • Spasticity is the most common abnormality of muscle seen in patients with cerebral palsy. The hallmark feature of spasticity is velocity-dependent stiffness of the muscle in proportion to the rate of muscle stretch, indicating a loss of central nervous system inhibition. • The increased muscle tone can induce abnormal movement patterns and frequently leads to the progressive development of muscle-tendon contractures and skeletal abnormalities, including torsional bone deformities and joint instability. • Surgical results are optimized when the timing of surgery is delayed until children have reached a functional “plateau.” At this point, the child has exhausted nonsurgical measures (physical therapy, orthoses, and pharmacologic spasticity management), has failed to demonstrate significant improvement over a 6-month follow-up period, and experiences significant functional impairments affecting ambulation and activities of daily living. • Gait analysis is an important component of the surgical decision-making algorithm for children with cerebral palsy. Quantitative gait analysis can provide objective information regarding deviations in three-dimensional joint kinematics involving multiple joints simultaneously and often provides additional information to the surgeon beyond that ascertained by physical examination alone. • Stiff-knee gait, which was previously described by Sutherland and Davids (1993) and represents the delayed and decreased dynamic knee flexion amplitude during the swing phase of the gait cycle, was seen across three of the four gait patterns described by Rhodda et al. (2004). As a result, it was considered to be a specific knee pattern but not a specific gait pattern. • In light of these specific gait patterns and their implications for treatment affecting functional outcomes, it is important for the treating orthopedic surgeon to carefully examine the hip and ankle when considered knee surgery in children with cerebral palsy. • The patient is placed in supine, with the pelvis positioned such that the anterior superior iliac spine (ASIS) is vertically aligned with the posterior superior iliac spine (PSIS), and lumbar lordosis is reduced. • One hip is flexed to 90° and the contralateral leg is assessed in full extension. • Any flexion of the contralateral leg indicates the presence of a hip flexion contracture. • If there is a concomitant knee flexion contracture, the patient is positioned so that the leg extends beyond the end of the examination table to accommodate the knee flexion contracture. • The patient is positioned in supine with one hip flexed to 90° and the contralateral leg extended. • Initially the ipsilateral knee is flexed to greater than 90° and then slowly the knee is extended until the first endpoint of resistance is felt and the pelvis begins to “rock”; the measurement (in degrees) lacking full extension is the KPA (Fig. 3). • The unilateral KPA is a measure of “functional hamstring contracture.” Functional KPA ranges from 0 to 49° (Katz et al., 1992); angles greater than 50° require surgical intervention. • The bilateral KPA is determined with the contralateral hip flexed until the ASIS and PSIS are in a vertical line, decreasing lumbar lordosis and pelvic tilt. The bilateral KPA gives a measure of “true hamstring contracture.” • The difference between the unilateral and the bilateral KPA is the “hamstring shift.” Hamstring shift greater than 20° indicates significant anterior pelvic tilt from (Delp et al., 2006):
Knee Surgery for Children with Cerebral Palsy
Introduction
 Children with cerebral palsy demonstrate three primary abnormalities of gait: (1) loss of selective motor control, (2) impaired balance, and (3) abnormal muscle tone.
Children with cerebral palsy demonstrate three primary abnormalities of gait: (1) loss of selective motor control, (2) impaired balance, and (3) abnormal muscle tone.
 Different gait patterns involving the knee have been described in ambulatory children with cerebral palsy. Most recently, Rhodda et al. (2004) identified four gait patterns in children with spastic diplegia and outlined surgical and nonsurgical treatment for each pattern (Fig. 1).
Different gait patterns involving the knee have been described in ambulatory children with cerebral palsy. Most recently, Rhodda et al. (2004) identified four gait patterns in children with spastic diplegia and outlined surgical and nonsurgical treatment for each pattern (Fig. 1).
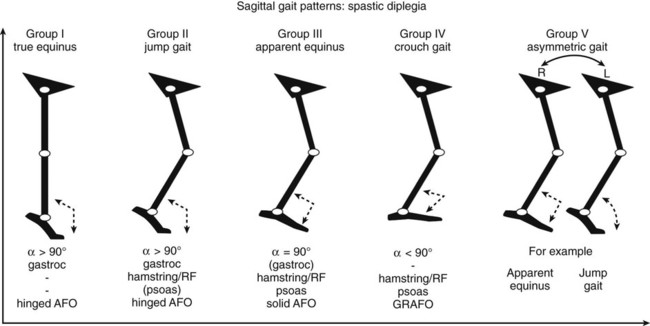
 True equinus gait occurs when the ankle is fixed in equinus but the knee, hip, and pelvis demonstrate a normal dynamic range of motion.
True equinus gait occurs when the ankle is fixed in equinus but the knee, hip, and pelvis demonstrate a normal dynamic range of motion.
 Surgical treatment of knee pathology in children with cerebral palsy rarely involves isolated muscle-tendon lengthening. This procedure highlights two of the surgical techniques commonly employed to treat knee pathology relative to the observed gait disturbances in children with cerebral palsy: hamstring lengthening and distal rectus femoris transfer (see Knee Surgery in Children with Cerebral Palsy II).
Surgical treatment of knee pathology in children with cerebral palsy rarely involves isolated muscle-tendon lengthening. This procedure highlights two of the surgical techniques commonly employed to treat knee pathology relative to the observed gait disturbances in children with cerebral palsy: hamstring lengthening and distal rectus femoris transfer (see Knee Surgery in Children with Cerebral Palsy II).
Examination/Imaging
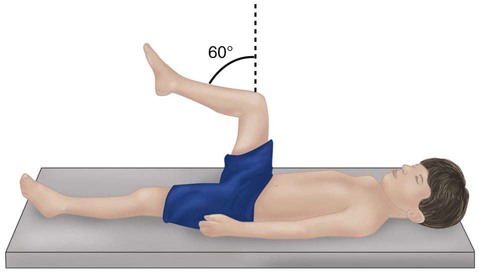
 Observational gait analysis is important in assessing which of the four gait patterns is present.
Observational gait analysis is important in assessing which of the four gait patterns is present.
 The hip is examined for the presence of hip flexion contracture with the Thomas test.
The hip is examined for the presence of hip flexion contracture with the Thomas test.
 The knee is examined for hamstring tightness and the presence of fixed knee flexion contracture.
The knee is examined for hamstring tightness and the presence of fixed knee flexion contracture.
 The knee-popliteal angle (KPA) is an effective tool to assess hamstring length (Fig. 2).
The knee-popliteal angle (KPA) is an effective tool to assess hamstring length (Fig. 2).

Surgical Anatomy
 The semitendinosus, gracilis, and semimembranosus make up the medial-side hamstring muscles that commonly insert onto the pes anserinus of the proximal medial tibia (Fig. 4).
The semitendinosus, gracilis, and semimembranosus make up the medial-side hamstring muscles that commonly insert onto the pes anserinus of the proximal medial tibia (Fig. 4).
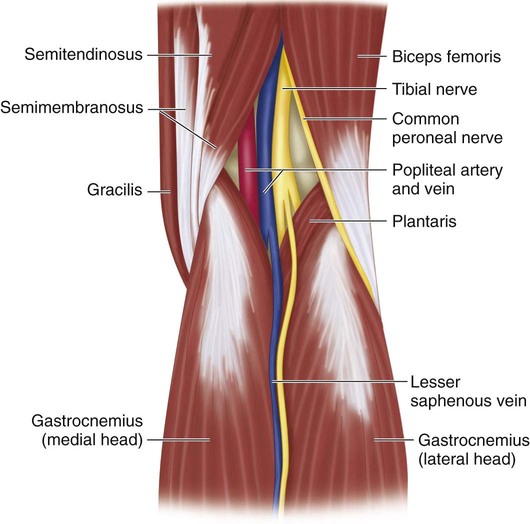
 The biceps femoris lies on the lateral border of the popliteal fossa. This tendon can be palpated proximal to the popliteal crease. Medial to the biceps femoris (lateral to medial) lie the common peroneal nerve, tibial nerve, popliteal vein, and popliteal artery (see Fig. 4).
The biceps femoris lies on the lateral border of the popliteal fossa. This tendon can be palpated proximal to the popliteal crease. Medial to the biceps femoris (lateral to medial) lie the common peroneal nerve, tibial nerve, popliteal vein, and popliteal artery (see Fig. 4).
 The common peroneal nerve lies along the posterior/medial border of the biceps femoris and can be difficult to isolate from the muscle-tendon junction of the biceps femoris in very contracted knees (see Fig. 4).
The common peroneal nerve lies along the posterior/medial border of the biceps femoris and can be difficult to isolate from the muscle-tendon junction of the biceps femoris in very contracted knees (see Fig. 4).
Portals/Exposures
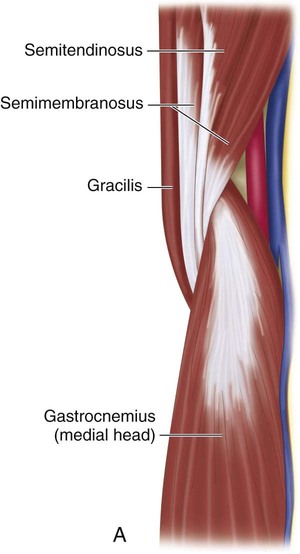
 A single incision, 3–6 cm in length, just medial or lateral to the palpable semitendinosus tendon at the mid- to distal third of the posterior thigh can be used to access all the hamstring tendons (Fig. 5).
A single incision, 3–6 cm in length, just medial or lateral to the palpable semitendinosus tendon at the mid- to distal third of the posterior thigh can be used to access all the hamstring tendons (Fig. 5).

 Sharp dissection through skin and electrocautery through subcutaneous tissue minimize blood loss.
Sharp dissection through skin and electrocautery through subcutaneous tissue minimize blood loss.
Procedure
Step 1
 The muscle-tendon junction of the semitendinosus is palpated. The sheath of the tendon is incised using a #15 blade or electrocautery.
The muscle-tendon junction of the semitendinosus is palpated. The sheath of the tendon is incised using a #15 blade or electrocautery.
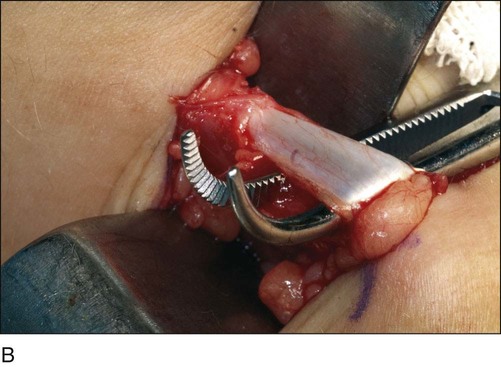
 A right-angle clamp is placed around the tendon from lateral to medial to prevent inadvertent injury to the neurovascular bundle (Fig. 6A and 6B).
A right-angle clamp is placed around the tendon from lateral to medial to prevent inadvertent injury to the neurovascular bundle (Fig. 6A and 6B).
 Electrocautery is used to amputate the semitendinosus at the level of the musculotendinous junction.
Electrocautery is used to amputate the semitendinosus at the level of the musculotendinous junction.
Related posts:
 4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
32: Patellar Instability: Lateral Release and Medial Plication
31: Discoid Lateral Meniscus
39: Open Reduction and Internal Fixation of Tibial Tubercle Fractures
59: Posterior Instrumented Reduction and Fusion for Spondylolisthesis
4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
32: Patellar Instability: Lateral Release and Medial Plication
31: Discoid Lateral Meniscus
39: Open Reduction and Internal Fixation of Tibial Tubercle Fractures
59: Posterior Instrumented Reduction and Fusion for Spondylolisthesis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


33: Knee Surgery for Children with Cerebral Palsy
























