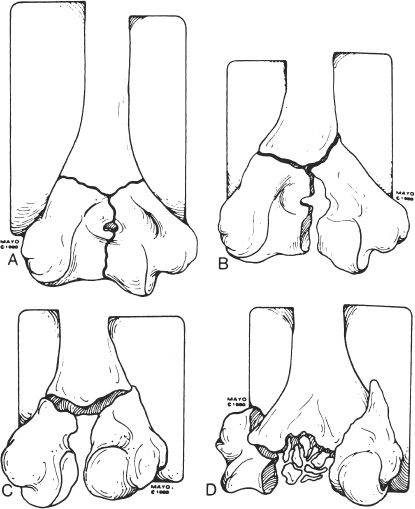
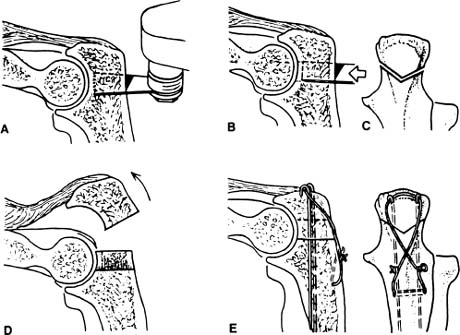
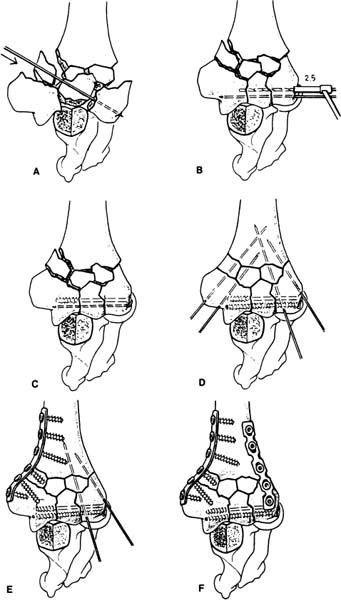
Case 33 A 23-year-old right-hand-dominant man presents with a 1-day history of left elbow pain and swelling following an altercation in which he was struck with a baseball bat on the elbow. He denies any other injuries and reports no significant numbness or tingling in his ipsilateral hand. His range of motion is severely limited secondary to pain. He also has crepitation with passive range of motion of the elbow. There is moderate swelling and contusion, but no significant lacerations. He is neurovascularly intact. Figure 33–1. Anteroposterior (AP) (A) and lateral (B) radiographs demonstrate an intercondylar distal humerus fracture. 1. Olecranon fracture 2. Distal humerus fracture 3. Radial head fracture 4. Elbow dislocation An anteroposterior (AP) and lateral radiograph are obtained (Fig. 33–1). Intercondylar Distal Humerus Fracture. Clinical examination and radiographs confirm a comminuted distal humerus fractures with intraarticular extension. Neurovascular examination is normal, and emphasis must be placed on a thorough evaluation of these structures. Not uncommonly, neurologic or vascular injury occurs with these high-energy fracture patterns. The goal of treatment is to reestablish articular congruity, attain acceptable alignment, and provide rigid fixation so as to allow immediate motion. The great majority of these patients require open reduction and internal fixation. Comminution of the bony fragments is not uncommon and loss of bony continuity allows for significant displacement of the fracture fragments because of unopposed muscular forces. Good-quality AP and lateral radiographs are essential in the accurate evaluation in these fracture patterns. Significant fracture displacement and comminution are generally present, sometimes making interpretation of the X-rays difficult. Computed tomography (CT) scanning can be very helpful in these situations. A number of classification schemes have been developed to further define these fracture patterns. The AO classification distinguishes extraarticular from intraarticular fractures and varies according to fracture fragment comminution (Fig. 33–2). Figure 33–2. (A) Type I nondisplaced intercondylar fracture. (B) Type II displaced but rotationally correct T-condylar fracture. (C) Type III fractures are displaced and rotated. (D) Type IV fractures are displaced, rotated, and significantly comminuted. (Reprinted from Rockwood C Jr, et al. Fractures in Adults. Philadelphia: Lippincott-Raven, 1996. With permission.) Displaced intercondylar distal humerus fractures in young adults must be reapproximated in as near-normal alignment as can be achieved with maximum stability. Fracture fragment stability allows for immediate motion, which is imperative in optimizing range of motion following this severe injury. The authors prefer AO plate and screw fixation of both the medial and lateral columns, with plates placed at 90-degree angles to each other. The patient is placed in the lateral decubitus position and a straight posterior incision made. Isolation and protection of the ulnar nerve is important and should be accomplished first. When significant articular extension and comminution is present, the authors prefer a transolecranon osteotomy technique (Fig. 33–3). Following a completion of the olecranon osteotomy, the medial and lateral columns are exposed, as is the distal articulation of the humerus. The order of fracture fragment fixation depends on the individual fracture pattern. However, the intraarticular portion usually requires fixation first. This is particularly true when the articular component of the fracture is significantly comminuted. However, there are times when one of the columns is minimally comminuted, and it is simpler to secure this column to the distal humerus first, and then reassemble the articular cartilage components of the fracture. Loss of articular cartilage can be accepted, but incongruity cannot. AO cannulated screws are valuable in reconstructing the articular fracture fragments. However, lag screws are not used in comminuted fractures because they change the normal articular configuration and make for a too-narrow, incongruous distal humeral articulation. Kirschner wires (K-wires) are valuable for provisional fixation as well. Also, as these fractures generally have significant degrees of comminution, the iliac crest is routinely prepped and draped at the time of surgery to provide for bone graft, if necessary. Figure 33–3.. (A–E) A chevron-type olecranon osteotomy can be employed for exposure of distal humerus intraarticular fractures. (Reprinted from Rockwood C Jr, et al. Fractures in Adults. Philadelphia: Lippincott-Raven, 1996. With permission.) Figure 33–4. (A) The most common sequence for fracture fixation of intercondylar distal humerus fractures begins with Kirschner-wire provisional stabilization. (B) Cannulated AO screw fixation of the articular fracture fragments is achieved. (C) Articular fracture fragment stabilization allows for reduction of the distal humerus. (D) Following reduction, percutaneous Kirschner-wire fixation temporizes the reduction. (E) Depending on the fracture configuration, medial columnar plate fixation is achieved. (F) Lateral columnar plate fixation placed at 90 degrees completes the fixation of the fracture. (Reprinted from Rockwood C Jr, et al. Fractures in Adults. Philadelphia: Lippincott-Raven, 1996. With permission.) • AO cannulated screws are very helpful in realigning the articular fracture fragments, as the cannulated guide wire provides temporizing fixation, eliminating the need for K-wire stabilization in these articular fracture fragments prior to screw placement. • Be careful to restore the normal 30-degree anterior angulation of the distal portion of the humeral condyles, as fixation in too much extension will severely limit motion postoperatively.
History and Physical Examination

Differential Diagnosis
Radiologic Findings
Diagnosis
Surgical Management
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


