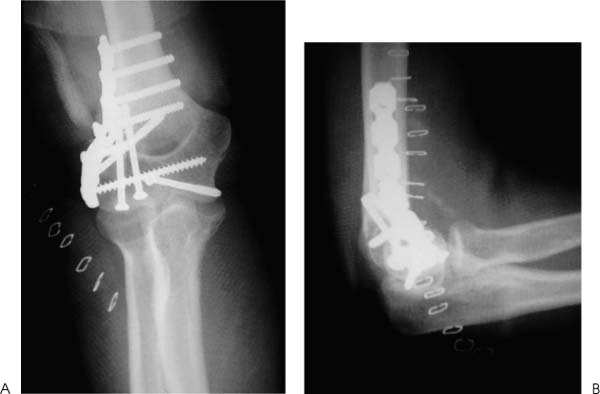
Case 32 A 60-year-old woman presents several hours after tripping in a hole and falling onto her extended elbow. She complains of pain and swelling of the elbow, as well as crepitation through a range of motion. She denies any numbness in her upper extremity or any other injury. Range of motion is limited to 60 to 85 degrees. She has moderate crepitation and pain through this range of motion. The arm is neurovascularly intact. Figure 32–1. Anteroposterior (AP) (A) and lateral (B) radiographs of a comminuted lateral condyle fracture. 1. Intercondylar distal humerus fracture 2. Supracondylar distal humerus fracture 3. Lateral condyle fracture 4. Elbow dislocation PEARLS • Ectopic bone formation is a common postoperative complication following comminuted elbow fractures, and routine prophylaxis for ectopic bone is recommended in these cases. • Significant comminution is often found at the time of fracture fixation, making anatomic reduction difficult if not impossible. It is extremely important that the normal articular dimensions of the distal humerus be restored, and for this reason, gaps between the articular surfaces may persist after fixation. Nevertheless, narrowing of the articular surfaces of the distal humerus will result in incongruency of the radio-capitellar articulation. An anteroposterior (AP) and lateral radiograph are obtained (Fig. 32–1). Lateral Condyle Fracture. Pain, swelling, and crepitation point toward a diagnosis of a distal humerus fracture. Radiographs confirm a highly comminuted lateral condyle fracture. Note the significant proximal displacement of the articular portion of the lateral condyle. This demonstrates the extreme valgus opening that probably occurred at the time of injury. Also, significant subluxation of the elbow joint has occurred due loss of articular congruity and ligamentous stability. Open reduction and internal fixation is the preferred approach in this situation. Any subluxation will significantly compromise nonoperative treatment. Also, the marked fracture displacement will result in malunion or nonunion. The patient is placed in a supine position and the arm placed on an arm board. A lateral arthrotomy is made. Care is taken to minimize the soft tissue disruption, as vascularity of these highly comminuted fragments may be jeopardized. The marked comminution of this fracture fragment will necessitate plate fixation in conjunction with screws to reapproximate the capitellar component of the fracture fragment (Fig. 32–2). Following fracture fixation, an assessment of range of motion as well as elbow and fracture stability should be carried out. The capsular disruption laterally is carefully repaired with absorbable sutures. The skin is closed in a normal fashion and a soft dressing applied. Figure 32–2. AP (A) and lateral (B) radiographs demonstrate good reduction and stabilization of this highly comminuted lateral condyle fracture. Early range of motion is imperative in all articular elbow fractures. Although comminution of this fracture may limit the aggressiveness of exercises, immediate range of motion is instituted. By 4 weeks postoperatively the patient’s range of motion was 15 to 120 degrees with full supination and pronation. AP and lateral radio-graphs taken 4 weeks after surgery confirm the maintenance of the reduction, but demonstrate ectopic bone formation in and around the anterior elbow capsule (Fig. 32–3). By 10 weeks postoperatively the patient’s range of motion was 10 degrees extension lag to full flexion with full supination and pronation. There was no instability to elbow testing, and she was allowed to return to full activities as tolerated. Forces applied to the posterior border of the proximal ulna are generally concentrated in the trochlear groove. When forces are applied centrally, both condyles may be wedged apart, producing an intercondylar fracture. If the force is applied eccentrically, fracture of either the medial or lateral condyle may occur. This case represents an extreme valgus force that generated a comminuted lateral condyle fracture with significant displacement. Figure 32–3. AP (A) and lateral (B) radiographs demonstrate ectopic bone formation 1 month following open reduction and internal fixation of a highly comminuted lateral condyle fracture. • Lateral condyle fractures are often comminuted, making fracture fixation a challenge. However, adequate stability is required for early motion. This often requires the use of a plate and screws construct. Inadequate or tenuous fixation is likely to fail, compromising motion recovery and even potentially ulnohumeral congruency. • Early range of motion is extremely important after open reduction and internal fixation of a lateral condyle fracture. Immobilization after surgery is very likely to result in significant loss of motion and is discouraged for all but the most severe fractures. • Additional injuries to the ligamentous stabilizers about the elbow often occur at the time of lateral condyle fracture. Both lateral ulnar collateral ligament injuries and medial ulnar collateral ligament injuries are common. An assessment of elbow stability following fracture fixation is important as acute repair of these ligamentous structures may be required if a high degree of instability persists following fracture fixation.
History and Physical Examination

Differential Diagnosis
Radiologic Findings
Diagnosis
Surgical Management
Postoperative Management
Discussion

Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


