• Acute deformity correction can be performed with subsequent gradual distraction for lengthening at the same osteotomy site. • Double femoral osteotomies can be performed for deformity correction at one site and lengthening at the second site. • Figure 1 shows an example of a patient with congenital femoral deficiency that is undergoing a femoral lengthening. A double-level osteotomy has been performed for acute deformity correction both proximally and distally with concurrent lengthening at the distal osteotomy site. Pitfalls • Congenital femoral deficiency • Juvenile rheumatoid arthritis • Hemihypertrophy: Klippel-Trénaunay syndrome • Developmental dysplasia/dislocation of the hip, slipped capital femoral epiphysis, and Legg-Calvé-Perthes disease Controversies • Severe deformities requiring extensive lengthening • LLD less than 5 cm in the skeletally immature patient • LLD less than 5 cm in the skeletally mature patient • Concurrent contractures or joint/bony abnormalities must be documented. • Concurrent joint instabilities and ligamentous deficiencies must be documented. • Malalignment and malorientation tests are performed to determine concurrent deformity and location of deformity. • Limb lengths are assessed (the pelvis should be leveled with blocks and the number of blocks noted on the radiograph). • The radiographs are checked for fixed flexion deformity of the knee. • A malorientation test is performed to determine the presence and location of sagittal plane deformity. • The radiographs are checked for joint subluxation (significant anterior-posterior instability). • Significant dysplasia will result in increased risk of hip dislocation. • Significant dysplasia requires pelvic osteotomy prior to femoral lengthening (Dega osteotomy, triple osteotomy, periacetabular osteotomy). • This structure will be penetrated by the laterally placed half-pins. • If a preoperative contracture is present, then a prophylactic release is required at the time of surgery. • These nerves are not directly at risk during the external fixation application or osteotomy. • Rapid lengthening or concurrent deformity correction can place tension on the neural elements. • Significant instability will result in increased risk of joint subluxation or dislocation. • Severe knee instability should be addressed with ligamentous reconstruction and patella realignment prior to femoral lengthening. • This marks the limb’s mechanical axis. • If the mechanical axis runs through the center of the knee joint, then a straight lengthening can be performed without concurrent deformity correction. • If an abnormal mechanical axis is present, then preoperative planning is required to determine the level of the deformity.
Femoral Lengthening with External Fixation
Indications
 Femoral shortening with or without concurrent limb deformity
Femoral shortening with or without concurrent limb deformity

Etiologies
 Severe concurrent deformities of the hip and knee—Joint realignment and reconstruction prior to lengthening.
Severe concurrent deformities of the hip and knee—Joint realignment and reconstruction prior to lengthening.
 Type V growth pattern with upward slope–plateau–downward slope with improvement without intervention.
Type V growth pattern with upward slope–plateau–downward slope with improvement without intervention.
 Final LLD should be assessed at skeletal maturity and then corrected.
Final LLD should be assessed at skeletal maturity and then corrected.
 LLD resulting from residual hip deformity may be treated with proximal femoral/hip osteotomies that impart length with concurrent realignment: proximal femoral valgus osteotomy (Wagner osteotomy); femoral neck lengthening osteotomy (Morscher osteotomy); surgical hip dislocation with subcapital osteotomy.
LLD resulting from residual hip deformity may be treated with proximal femoral/hip osteotomies that impart length with concurrent realignment: proximal femoral valgus osteotomy (Wagner osteotomy); femoral neck lengthening osteotomy (Morscher osteotomy); surgical hip dislocation with subcapital osteotomy.
Examination/Imaging
Physical Examination
 Range of motion of the hip, knee, and ankle joints
Range of motion of the hip, knee, and ankle joints
 Special consideration must be given to knee fixed flexion deformity. The cause (soft tissue contracture vs. bony deformity) must be determined.
Special consideration must be given to knee fixed flexion deformity. The cause (soft tissue contracture vs. bony deformity) must be determined.
 Clinical limb-length assessment
Clinical limb-length assessment
Radiographic Examination
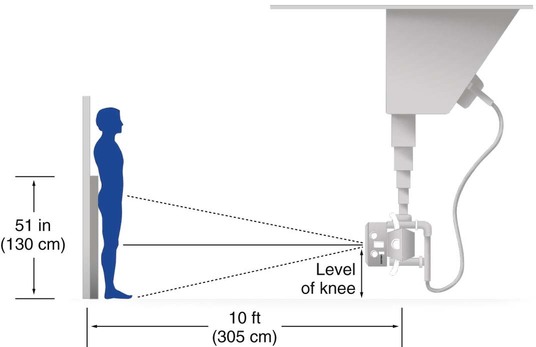
 Anteroposterior (AP) and lateral standing long-leg radiographs are obtained (taken at a distance of 10 feet using a 51-inch cassette) (Figs. 2 and 3).
Anteroposterior (AP) and lateral standing long-leg radiographs are obtained (taken at a distance of 10 feet using a 51-inch cassette) (Figs. 2 and 3).
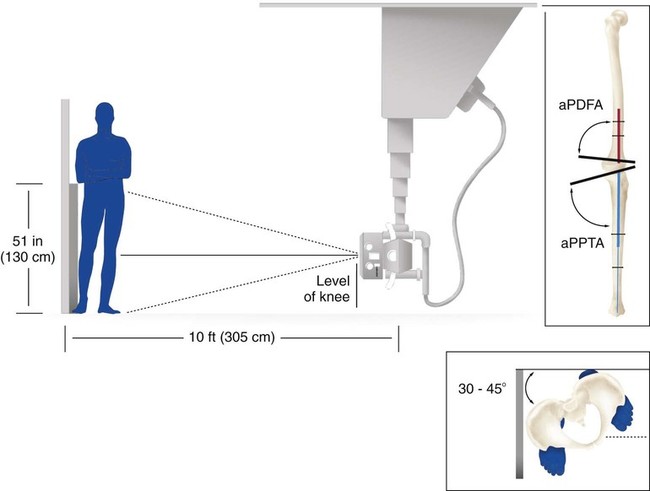
 Standing long-leg lateral radiographs (with maximum knee extension) are obtained (Fig. 4).
Standing long-leg lateral radiographs (with maximum knee extension) are obtained (Fig. 4).

Surgical Anatomy
 Tensor fascia lata/iliotibial band (ITB)
Tensor fascia lata/iliotibial band (ITB)
 At the end of the procedure, the knee must be maximally flexed to stretch/tear the fascia lata around the half-pins.
At the end of the procedure, the knee must be maximally flexed to stretch/tear the fascia lata around the half-pins.
 The sciatic nerve is tethered as the common peroneal nerve enters the lateral compartment of the lower leg.
The sciatic nerve is tethered as the common peroneal nerve enters the lateral compartment of the lower leg.
 Peroneal nerve tension or irritation initially will result in pain on the anterior aspect of the lower leg and dorsum of the foot and altered sensation in the first web space. Late findings include weakness of dorsiflexors or footdrop. Young patients will often hold the toes up with their hands or continuously rub their foot. Treatment involves slowing the rate of distraction, allowing the hip to extend and the knee to flex, and decompression of the peroneal nerve.
Peroneal nerve tension or irritation initially will result in pain on the anterior aspect of the lower leg and dorsum of the foot and altered sensation in the first web space. Late findings include weakness of dorsiflexors or footdrop. Young patients will often hold the toes up with their hands or continuously rub their foot. Treatment involves slowing the rate of distraction, allowing the hip to extend and the knee to flex, and decompression of the peroneal nerve.
 A contracted ITB will result in rotatory subluxation of the knee joint with concurrent knee flexion contracture and patella dislocation.
A contracted ITB will result in rotatory subluxation of the knee joint with concurrent knee flexion contracture and patella dislocation.
 Contracted hamstrings will result in posterior subluxation/dislocation of the knee joint.
Contracted hamstrings will result in posterior subluxation/dislocation of the knee joint.
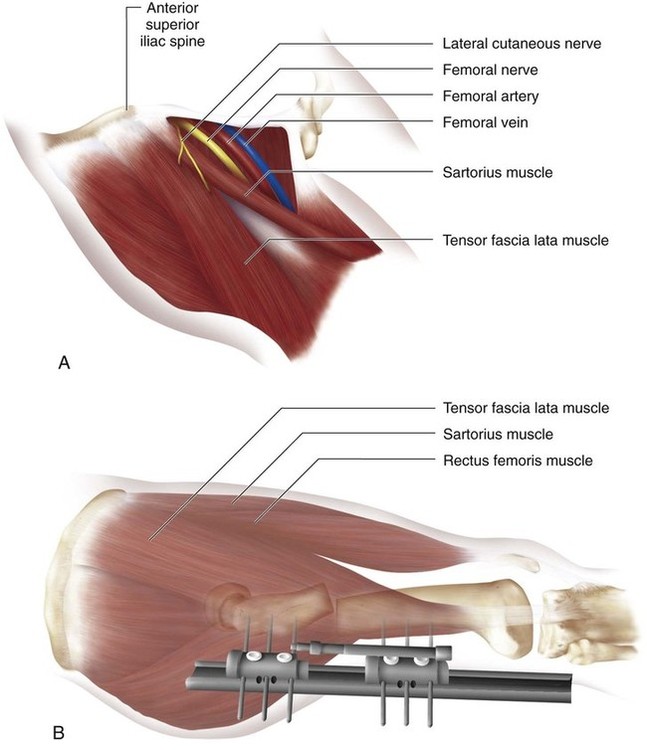
 Figure 5 illustrates the neurovascular structures of the proximal anterior thigh region that are located medial to the sartorius muscle (Fig. 5A) and the typical placement of the monolateral external fixator for femoral lenghthening (Fig. 5B). Note that the external fixation pins are placed from the lateral position posterior to the tensor fascia lata muscle and away from the neurovascular elements.
Figure 5 illustrates the neurovascular structures of the proximal anterior thigh region that are located medial to the sartorius muscle (Fig. 5A) and the typical placement of the monolateral external fixator for femoral lenghthening (Fig. 5B). Note that the external fixation pins are placed from the lateral position posterior to the tensor fascia lata muscle and away from the neurovascular elements.
Positioning
 The patient is placed supine on a radiolucent table that allows visualization from the hips to the ankles.
The patient is placed supine on a radiolucent table that allows visualization from the hips to the ankles.
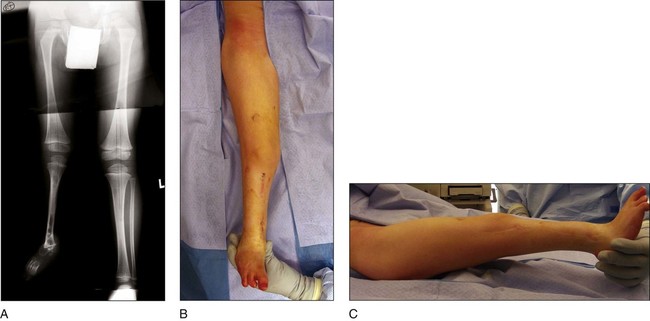
 Figure 6 shows a patient with fibular hemimelia with significant concurrent congenital femoral deficiency (Fig. 6A). The patient’s lower extremity is draped to allow entire access from the pelvis to the foot (Fig. 6B and 6C).
Figure 6 shows a patient with fibular hemimelia with significant concurrent congenital femoral deficiency (Fig. 6A). The patient’s lower extremity is draped to allow entire access from the pelvis to the foot (Fig. 6B and 6C).
Procedure: External Fixator Placement
Step 1
 The limb is held patella forward and the patient is adjusted so a line on the radiopaque grid runs through the center of the hip joint.
The limb is held patella forward and the patient is adjusted so a line on the radiopaque grid runs through the center of the hip joint.
 The osteotomy site will be influenced by the level of the center of rotation of angulation (CORA) of the deformity.
The osteotomy site will be influenced by the level of the center of rotation of angulation (CORA) of the deformity.Related posts:
 4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
32: Patellar Instability: Lateral Release and Medial Plication
31: Discoid Lateral Meniscus
39: Open Reduction and Internal Fixation of Tibial Tubercle Fractures
59: Posterior Instrumented Reduction and Fusion for Spondylolisthesis
4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
32: Patellar Instability: Lateral Release and Medial Plication
31: Discoid Lateral Meniscus
39: Open Reduction and Internal Fixation of Tibial Tubercle Fractures
59: Posterior Instrumented Reduction and Fusion for Spondylolisthesis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






























































