• Figure 3A demonstrates a 12-year-old female presenting with unilateral Blount disease, including lateral ligamentous laxity and thrust. There is no concomitant femoral valgus or varus deformity. • Twelve months following guided growth of the tibia, her mechanical axis is neutral, the lateral laxity and thrust are resolved, and the 8-plate was removed (Fig. 3B). Treatment Options • Phemister permanent epiphysiodesis (open vs. percutaneous)—While no hardware is implanted, this is an unforgiving and irreversible technique whereby the physis is surgically ablated. Errors in timing or follow-up may result in iatrogenic deformity requiring an osteotomy for salvage. • Blount staples—Practiced for 6 decades, problems with staple migration, bending, and breakage have led to its declining popularity. • Metaizeau (PETS) procedure—This uneccessarily violates the physis with large (6.5-mm) screws that may be difficult to remove. This is inapplicable in younger children and may not be reversible. It is not feasible to correct sagittal or oblique plane deformities.
Guided Growth—Hemiepiphysiodesis
Examination/Imaging
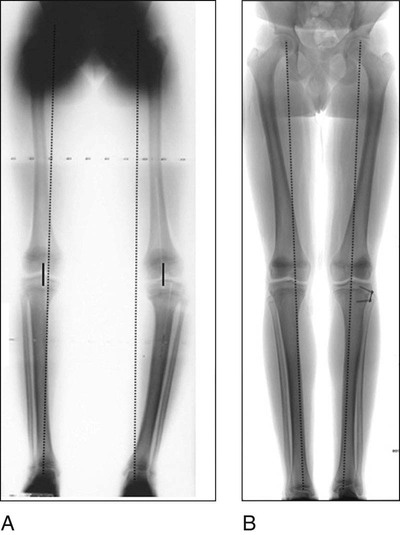
 A full-length anteroposterior (AP) standing teloroentgenogram of the legs is obtained with the patellae facing forward and the pelvis leveled as needed with a block under the foot of the shorter leg (Fig. 1). The other side is properly positioned with the patella neutral.
A full-length anteroposterior (AP) standing teloroentgenogram of the legs is obtained with the patellae facing forward and the pelvis leveled as needed with a block under the foot of the shorter leg (Fig. 1). The other side is properly positioned with the patella neutral.

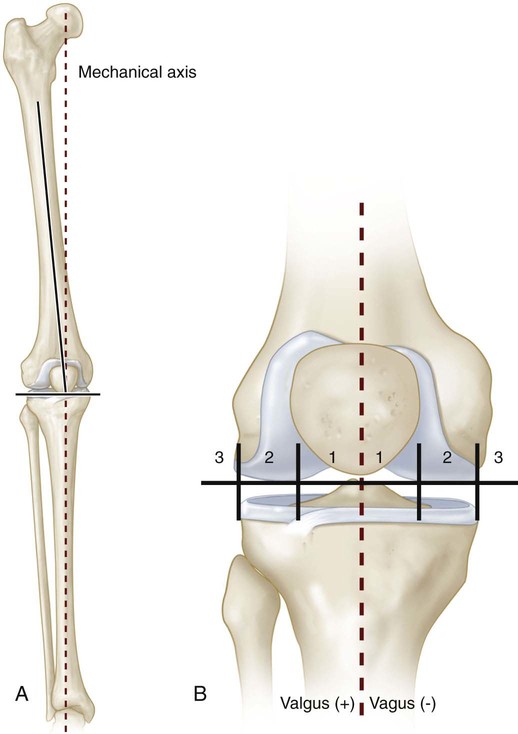
 On this frontal projection, the mechanical axis should bisect the knee, or at least fall within the central two quadrants (Fig. 2A). Dividing the knee into quadrants, the mechanical axis should fall within the central two quadrants (± zone 1). Zones 2 and 3 represent indications for guided growth to restore the axis to (or slightly past) neutral (Fig. 2B).
On this frontal projection, the mechanical axis should bisect the knee, or at least fall within the central two quadrants (Fig. 2A). Dividing the knee into quadrants, the mechanical axis should fall within the central two quadrants (± zone 1). Zones 2 and 3 represent indications for guided growth to restore the axis to (or slightly past) neutral (Fig. 2B).
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 28: Femur Fracture: Closed Reduction and Spica Cast
28: Femur Fracture: Closed Reduction and Spica Cast
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


22: Guided Growth—Hemiepiphysiodesis







