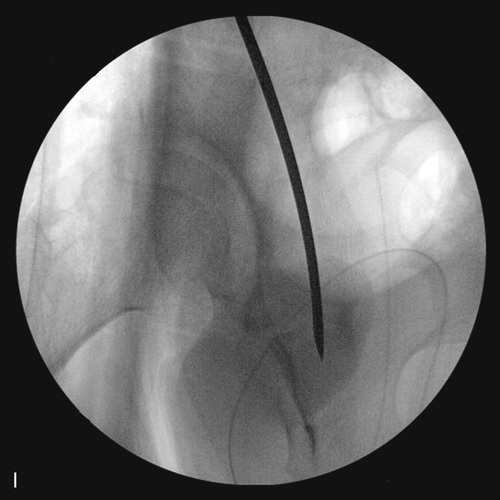
Manipulation and positioning of the acetabular fragment. J, A Shanz pin is placed just superior to the acetabulum. First, the fragment is positioned by disengaging the superior ramus to allow for medicalization of the hip joint center and to ensure adequate restoration or maintenance of version. The primary correction maneuver is forward rotation with slight tipping of the fragment medially. The radiographs should demonstrate four key points: 1. Lateral coverage; 2. Anterior coverage; 3. Medicalization; and 4. Normal version. K, This fluoroscopic view demonstrates overcorrection with excess medicalization and lateral coverage with a downturning sourcil. L, Following repositioning, the sourcil is horizontal with good lateral coverage, normal version, and normal medicalization with restoration of Shenton’s line.
Ganz Periacetabular Osteotomy
Operative Technique
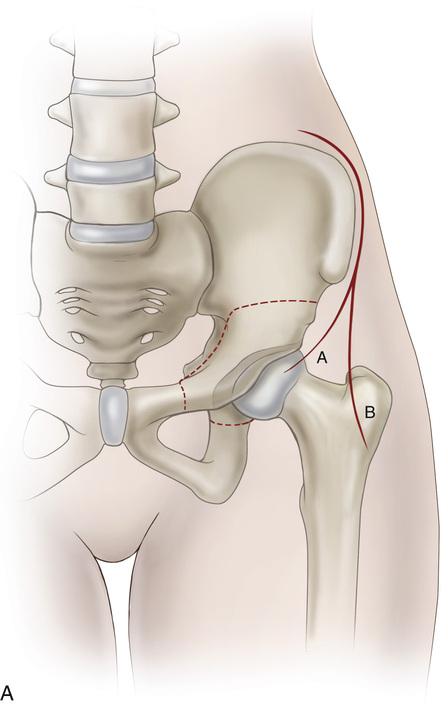
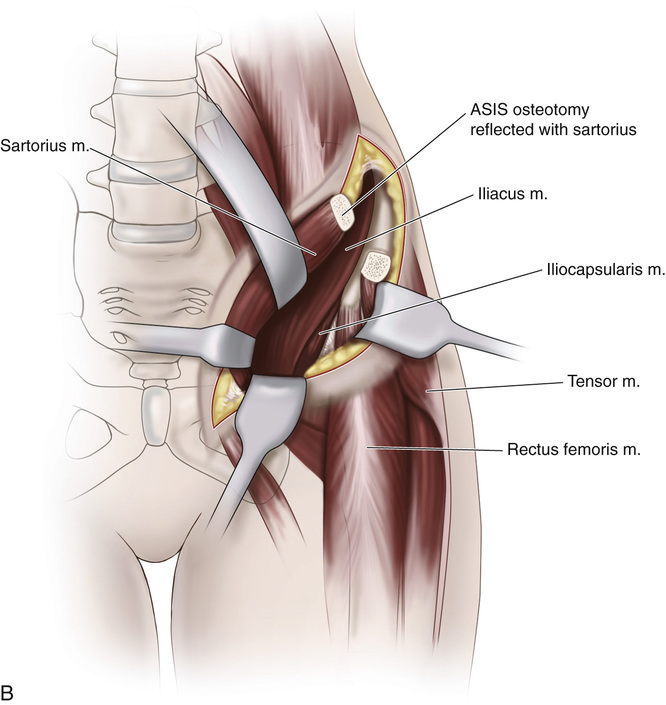
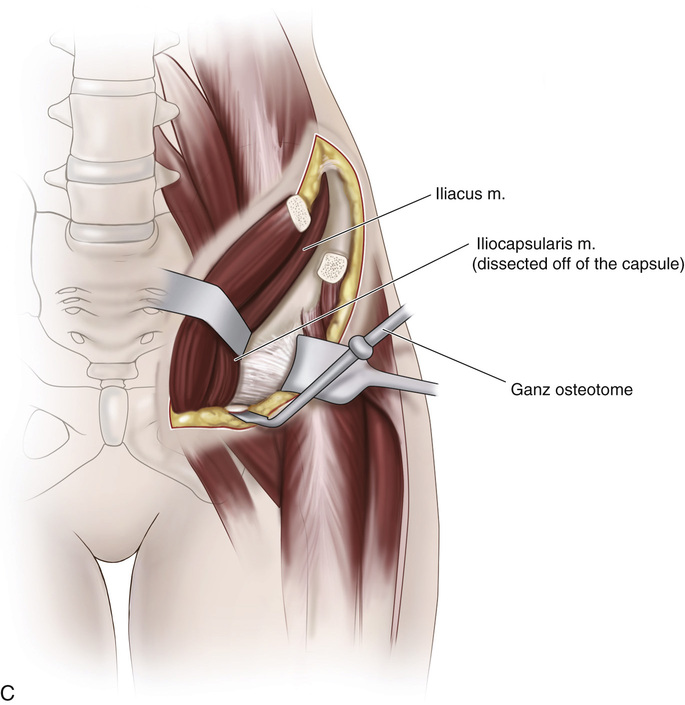
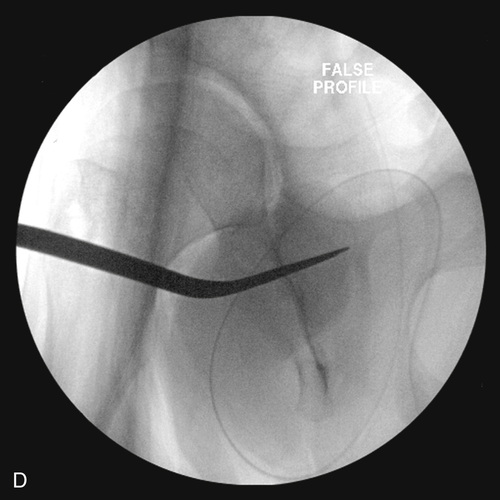
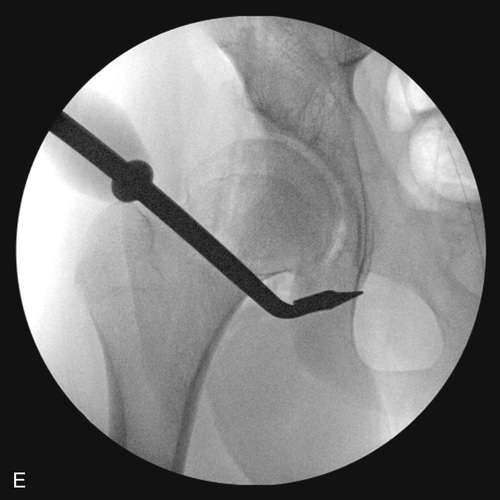
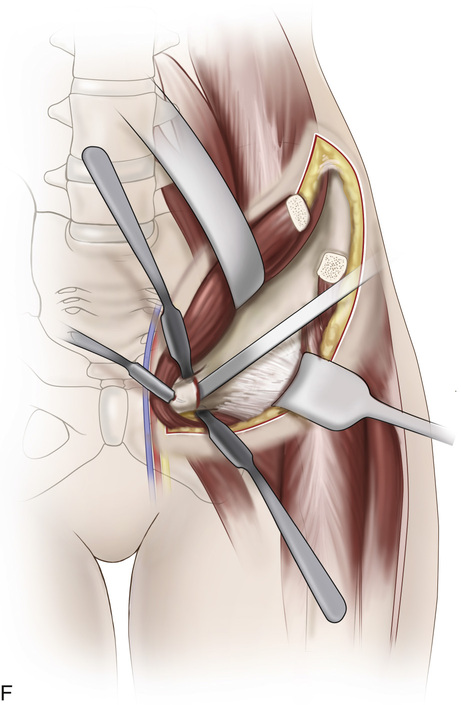
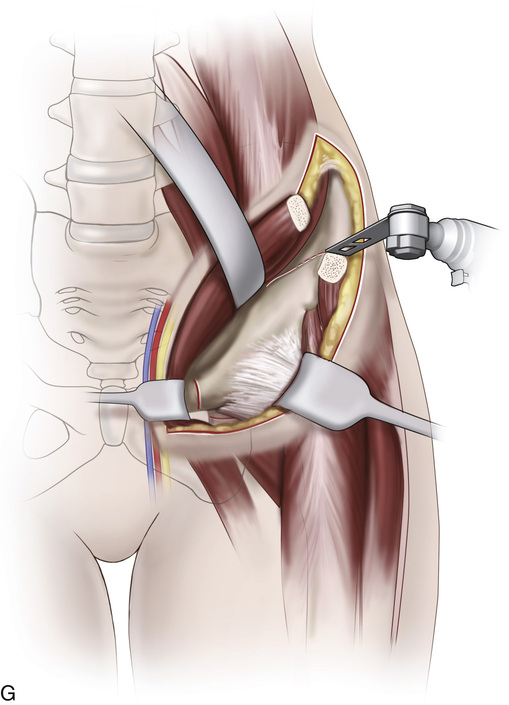
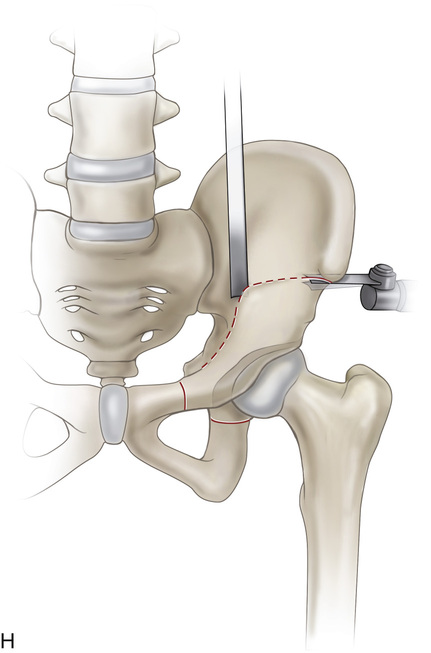
 A, Two types of incisions can be made. Both incisions track along the iliac crest until ending just over the anterior superior iliac spine (ASIS). A, The incision continues medially and distally and is used for the more straightforward PAO when previous surgery has not occurred and looking in the hip joint is not planned. B, The incision curves distally and laterally over an imaginary area over the tensor fascia lata and is used for more challenging hips and/or when an arthrotomy is planned. B, The fascia of the tensor fascia lata is incised, and the muscle is retracted laterally and the fascia medially. The sartorius and the fascia from the tensor fascia are retracted medially with the osteotomized anterior superior iliac spin. C, Ischial osteotomy. A soft tissue dissection is made between the direct head of the rectus muscle and the iliacus-ilicapsularis-iliopsoas muscle. Capsular exposure. The ilicapsularis muscle is sharply dissected off the capsule. D, A curved Mayo retractor is placed between the capsule and the psoas opening a window to allow the osteotome to enter. E, The ishial osteotomy is made beginning below the acetabulum and directed posteriorly under fluoroscopy using the AP and the false profile projections. F, The Superior ramus osteotomy. Soft tissue dissection first elevates the ileopectineal fascia over the pelvic brim and into the obturator foramen, and soft tissue retractors are placed circumferentially into the obturator. A sharp-tipped Homan is placed on the anterior aspect of the superior ramus. A straight osteotomy begins the osteotomy just medial to the ileopectineal eminence and is directed at 45 degrees from the horizontal to maintain a floor for the ileopsoas tendon. G, The innominate osteotomy. A small soft tissue window is made on the lateral aspect of the iliac wing and a smooth Homan is placed to protect the muscle. The osteotomy begins at the tip of the anterior superior iliac spine and is directed down to the floor ending just lateral to the pelvic brim. A fluoroscopic false profile image should be made to ensure this endpoint will allow for an adequate posterior column osteotomy. H, The posterior column osteotomy. A long-curved osteotomy with a rotation-controlling handle is used to make this cut. I, The false profile radiograph is used to ensure this cut is posterior to the acetabulum but anterior to the posterior edge of the posterior column.
A, Two types of incisions can be made. Both incisions track along the iliac crest until ending just over the anterior superior iliac spine (ASIS). A, The incision continues medially and distally and is used for the more straightforward PAO when previous surgery has not occurred and looking in the hip joint is not planned. B, The incision curves distally and laterally over an imaginary area over the tensor fascia lata and is used for more challenging hips and/or when an arthrotomy is planned. B, The fascia of the tensor fascia lata is incised, and the muscle is retracted laterally and the fascia medially. The sartorius and the fascia from the tensor fascia are retracted medially with the osteotomized anterior superior iliac spin. C, Ischial osteotomy. A soft tissue dissection is made between the direct head of the rectus muscle and the iliacus-ilicapsularis-iliopsoas muscle. Capsular exposure. The ilicapsularis muscle is sharply dissected off the capsule. D, A curved Mayo retractor is placed between the capsule and the psoas opening a window to allow the osteotome to enter. E, The ishial osteotomy is made beginning below the acetabulum and directed posteriorly under fluoroscopy using the AP and the false profile projections. F, The Superior ramus osteotomy. Soft tissue dissection first elevates the ileopectineal fascia over the pelvic brim and into the obturator foramen, and soft tissue retractors are placed circumferentially into the obturator. A sharp-tipped Homan is placed on the anterior aspect of the superior ramus. A straight osteotomy begins the osteotomy just medial to the ileopectineal eminence and is directed at 45 degrees from the horizontal to maintain a floor for the ileopsoas tendon. G, The innominate osteotomy. A small soft tissue window is made on the lateral aspect of the iliac wing and a smooth Homan is placed to protect the muscle. The osteotomy begins at the tip of the anterior superior iliac spine and is directed down to the floor ending just lateral to the pelvic brim. A fluoroscopic false profile image should be made to ensure this endpoint will allow for an adequate posterior column osteotomy. H, The posterior column osteotomy. A long-curved osteotomy with a rotation-controlling handle is used to make this cut. I, The false profile radiograph is used to ensure this cut is posterior to the acetabulum but anterior to the posterior edge of the posterior column.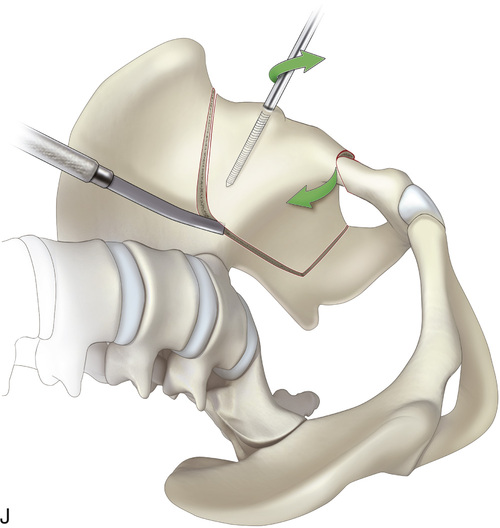


Related posts:
 23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


