(1)
Cirurgia Ortopèdica i Traumatologia, Fundació Hospital De Sant Celoni, Av. Hospital, 19, Sant Celoni, 08470, Spain
31.1 Introduction
The wrist is a complex joint that biomechanically transmits forces generated at the hand through to the forearm. The radial side of the wrist carries 80 % of the axial load and the ulnar side the remaining 20 % of the load. The incidence of wrist (and hand) injuries [1] in the sporting population is approximately 25 %.
The injuries are divided into four categories: overuse, nerve (and vascular), traumatic, and weight-bearing injuries. Overuse injuries are common in sports involving the hand and the wrist, such as racquet sports, golf, netball, basketball, and volleyball. Nerve injuries are more commonly compressive neuropathies and are seen with cyclists who may compress the ulnar nerve in Guyon’s canal. Traumatic injuries are the most common and due to either a fall on to the wrist, a direct blow, or combination of a rotatory and torsional force. The weight-bearing injuries are more specific to gymnastics and result from repetitive excessive compressive and rotational forces across the wrist.
Golf and racquet sports are played throughout the world, both at a professional level and for health and recreation. With regard to golf, it was estimated in 2001 that 37 million individuals played 518 million rounds in the United States alone [2]. Major racquet sports around the world consist of tennis, table tennis, squash, and badminton. Tennis is the most common racquet sport; it has been estimated that tens of millions play tennis in the United States alone, and sports such as badminton are popular in Sweden, with 680,000 participating at least once per week during the winter season. With the large numbers of individuals participating in such golf and racquet sports activities, it is understandable that associated injuries are recognized.
31.2 Etiology and Injury Mechanisms
Depending of the kind of sport in practice, we can find some different tendon lesion. A lot of studies have been done about, and the majority of them referred to golf and racquet sport.
31.2.1 Types of Injuries in Golf Players
The prevalence of golf injuries has ranged from 25 to 62 %, with individuals older than 50 years of age or with a low handicap (1–9) having a higher prevalence [2]. The prevalence of injuries of professional golfers has been reported to be as high as 88.5 %, probably related to the number of hours participating in the sport [2]. The etiology of golf injuries can include overuse, technical errors during swing, physical fitness deficiencies (aerobic, muscle strength, flexibility), no pregame warm-up, carelessness or lack of etiquette, and natural environmental conditions (uneven surface, thunderstorms). In amateur golfers, the three most common sites of injury are the thoracolumbar spine (27 %), elbow (26 %), and wrist and hand (16 %) [1]. For the professional golfer, the three most common sites are the wrist (27 %), lumbar spine (23 %), and shoulder (9 %) [1]. Lower extremity injuries are less common than spine or upper extremity injuries in either group [1]. Golf injuries can be considered as two groups: overuse (54.5 %) or acute trauma (45.5 %) [1].
The majority of wrist problems (29–67 % of all problems) involved the leading wrist (87 %). [3]
Symptoms can be described in a variety of anatomical location:
1.
Ulnar-sided problems: A cause of pain comprises extensor carpi ulnaris (ECU) tendinosis, ECU subluxation, and ulnar pain after hitting a “fat” shot (where too much turf is taken while playing a shot). ECU subluxation can be acute as a result of an unexpected impact with a tree root or object during a full shot.
2.
Radial-sided pain: de Quervain’s disease can occur also in the leading wrist, and it has been described an intersection syndrome in a player at the beginning of the season [3].
3.
Dorsal wrist pain: Some golfers have ganglia on the dorsum of the wrist, sometimes in the leading wrist and sometimes in the non-leading one. It has been also described [3] extensor tenosynovitis, dorsal rim impaction syndrome (a condition of hypertrophic radiolunate synovitis causing pain on loaded extension in the dorsal central area of the wrist).
The golf swing is traditionally divided into five phases (address, backswing, downswing, impact, and follow-through). The leading, non-dominant wrist (the left wrist for right-handed golfers) begins the golf swing in a position of ulnar deviation when addressing the ball. As the club is lifted away into the backswing, this wrist moves into radial deviation until it sits maximally radially deviated at the top of the backswing. At this point, the club changes direction to begin the downswing, and the leading wrist returns to ulnar deviation until impact. Several biomechanical works have studied the load transmission across the wrist and found an increased in distal ulnar loading with progressively increasing ulnar deviation [3].
31.2.2 Types of Injuries in Tennis Players
The biomechanics of a tennis swing have been extensively studied. In contrast, less has been described pertaining to the other major racquet sports of table tennis, squash, and badminton; however, certain aspects of the tennis swing can apply. The biomechanics of a tennis swing can be divided into three basic strokes: overhead or serve, forehand, and backhand. Significant forces are applied to the upper limb with hand speeds at ball impact approaching 47 miles per hour in world-class tennis players [2].
The tennis serve is composed of four stages: wind-up, cocking, acceleration, and deceleration and follow-through.
Forehand and backhand strokes consist of three stages: racquet preparation, acceleration, and follow-through. The wrist extensors are very active in every stroke. Of note, wrist extensors do not demonstrate increased activity with a single-handed backhand stroke compared with a double-handed backhand stroke.
In tennis players, injuries are typically from overuse or acute trauma.
Tendinitis and stenosing tenosynovitis have been described in association with almost all tendons in the wrist and hand. The mechanism is usually from chronic overstretching or recent initiations of an unaccustomed motion or activity. The symptoms are usually a vague pain radiating along the affected tendon into its insertion and occasionally affecting the joints over which tendons cross.
We subdivide wrist tendon lesion by its localization, dorsal or volar (Fig. 31.1):
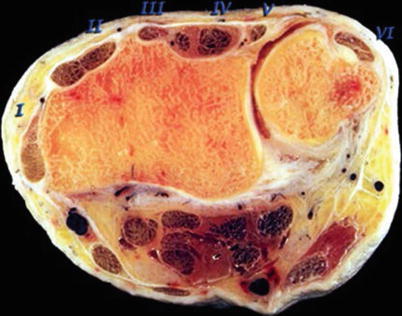
Fig. 31.1
The extensor compartments (with permission by Prof. Ivan Saenz Navarro. Hospital Clinic, Barcelona)
Dorsal:
De Quervain’s tenosynovitis
Intersection syndrome
Extensor insertional tenosynovitis
ECU lesions
Volar:
Flexor carpi radialis (FCR) tenosynovitis
Other tendons
31.3 Pathology
31.3.1 De Quervain’s Tenosynovitis
The most common form of stenosing tenosynovitis reported in racquet sports is de Quervain’s disease [4–7]. It consists of inflammation of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) as they pass through the first compartment at the level of the radial styloid. Often there are multiple slips of the APL. Repetitive ulnar deviation and grasp can inflame these tendons in this closed space resulting in pain with thumb use. Clinically there is swelling and tenderness along the radial aspect of the wrist. Filkenstein’s test is positive, with pain reproduced by having the patient tuck his thumb into the palm and then ulnarly deviate the wrist. This lesion may be bilateral in 30 % of the cases, and it exist a septum between the tendons in approximately 70 %.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


