Fig. 15.1
Wrist radiographs demonstrating wrist arthritis. (left) scapholunate advanced collapse (SLAC) Wrist Stage III/IV with stylo-scaphoid arthritis, radiocarpal arthritis, and joint space narrowing of the capitolunate junction. (right) scaphotrapeziotrapezoidal (STT) arthritis with joint space narrowing and sclerotic changes
We believe that magnetic resonance imaging (MRI) with an appropriate clinical history has a high sensitivity and specificity for imaging articular cartilage when confirmed by arthroscopic findings and clinical correlations. However, others refute the role of MRI as a diagnostic tool. Haims and colleagues concluded that wrist MRI (41 indirect MR arthrograms and 45 unenhanced [nonarthrographic] MR images) is not adequately sensitive or accurate for diagnosing cartilage defects in the distal radius, scaphoid, lunate, or triquetrum, as demonstrated compared to arthroscopic findings [20]. This was also supported by Multimer et al. who demonstrated that MRI and arthroscopy are not correlated and therefore arthroscopy continues to have a role in the diagnosis of an arthritic wrist [21]. While true for the radiologist that sees a rare MRI of the wrist, a trained muscuoloskeletal radiologist well-versed in wrist anatomy can be enormously helpful in treatment planning with an accurate read of the cartilage status of the wrist.
In cases of synovitis and ulnar-sided pathology, MRI remains a strong indicator for which areas need to be addressed with the arthroscope to treat successfully. Signs of synovitis, enhancement with bone erosion-like changes, and of bone marrow edema are strong indicators of an evolving arthritic disease process [22, 23].
MRI is also a sensitive method for excluding the diagnosis of early avascular necrosis and for evaluating the extent to which fibrocartilaginous repair tissue has formed postoperatively. These post-microfracture or cartilage repair procedures have been utilized to look at knee pathology post-surgery, and we have established the same protocols for wrist defects [20, 24].
Treatment Options
Conservative Management
Nonoperative measures for wrist arthritis are typically the first line of defense and are primarily aimed at relieving pain in the wrist. Rest in the form of splinting with removable thermoplastic splints constructed by a certified hand therapist may be useful during periods of exacerbation. The wrist is usually maintained in neutral or slight dorsiflexion, the functional position of the wrist. While providing pain relief, the disadvantages of splinting include stiffness and wrist weakness as a result of overuse or prolonged immobilization which should always be avoided. Therefore, splinting should be used in conjunction with alternative therapies such as exercise and occupational hand therapy.
Pharmacologic management should also be used during inflammatory periods to control pain and swelling. For patients with inflammatory arthritis, nonsteroidal anti-inflammatory drugs (NSAIDs) are indicated to assist in controlling inflammation and reducing synovitis. Topical NSAIDs have become increasingly popular in recent years to control acute and chronic symptoms. These eliminate the adverse, systemic complications associated with prolonged, oral NSAID use. Topical formulations can be compounded with ingredients such as muscle relaxants, calcium-channel blockers, anesthetics, and GABA-receptor blockers to provide a broader coverage of symptoms. Anti-rheumatic medications, including systemic steroids, methotrexate, and anti-tumor necrosis factor, are indicated for patients with RA and Allopurinol, a xanthine oxidase inhibitor, may be useful in patients with gouty arthritis of the wrist.
Steroid injections, with or without local anesthetic into the joint, may also be performed. Methylprednisolone acetate injection into the wrist can play a role in treating degenerate triangular fibrocartilage. Local steroid injections using a 1½″, 25- or 27-gauge needle when combined with local anesthetic may provide both a diagnostic and therapeutic effect. The effect of steroid injections are transient and therefore repeat injections may be needed. However, repeat injections should be used sparingly (our recommended maximum is two) due to the associated risk of soft tissue weakening and thinning of the cartilage in an already compromised joint.
Surgical Management
When conservative options have failed, arthroscopic intervention may be a viable option for some patients. Indications for the surgical management are dependent on the severity and the extent of wrist arthritis. MRI in conjunction with clinical assessment of the patient aids surgical decision-making. Arthroscopic procedures are more favorable compared to their parent open procedures due to less joint capsule and ligament damage. In general, arthroscopic procedures are safe procedures with no major complications being reported [25–27].
In the earliest stages, when the problems are mainly caused by carpal instability (i.e. pre-arthritic stage), the aim of the surgery is to restore the anatomic position and to correct the carpal instability to prevent degeneration. In the intermediate stages, when the patient has well-established arthritis but a well-preserved range of motion, no proven standard treatment has been established. The available options are geared toward less invasive procedures with fewer complexities such as synovectomy, abrasion chondroplasty, radial styloidectomy, and proximal row carpectomy via arthroscopic techniques. In the late stages of arthritis, a partial or total wrist arthrodesis, a PRC, or a total wrist arthroplasty may be contemplated. Patients with severe dorsal tenosynovitis have weakened tendons and are not usually candidates for arthroscopy due to the risk of tendon injury when establishing portals.
Arthroscopic synovectomy has become a well-described procedure. Aggressive arthroscopic debridement, including radial styloidectomy and partial resection of the scaphoid, has been reported. Resection of the lunate in patients with Kienböck’s disease may also be performed arthroscopically. In the DRUJ, arthroscopy can be used for debridement of the TFCC and for a modified Darrach procedure that involves distal ulna resection. Arthroscopic reconstructive procedures have been described for repair of the lunate-triquetrum ligament and ulnocarpal ligament complex, as well as for capsular placation. More recently, arthroscopy has seen increased use for the removal of single or multiple bones in the proximal carpal row and for partial wrist fusions, procedures that are traditionally performed using open techniques.
Arthroscopic Synovectomy
Arthroscopic synovectomy provides effective treatment of patients with RA, juvenile RA, systemic lupus erythematosus (SLE), and post-infectious arthritis when conservative measures have failed [4–6, 27]. Patients with posttraumatic joint contractures and septic arthritis of the wrist after failed systemic antibiotics and lavage also benefit from arthroscopic synovectomy. Patients requiring more extensive, open wrist procedures would not be an ideal candidate for arthroscopic synovectomy. The goal of the procedure is to decrease pain and improve joint function by excising the inflamed synovium and thereby removing or eliminating the effusion and inflammatory substrate.
The protocol for arthroscopic synovectomy in patients with RA was established by Adolfsson [4]. Indications include persistent joint symptoms following a 6 month course of pharmacologic treatment and the presence of radiographic changes of grade 0, I, or II according to the staging system by Larsen and colleagues [28]. Synovectomy for RA is indicated in the early stages of development when complete synovectomy is more feasible and has been shown to slow and even halt the progression of the disease [6, 29]. It allows for significant improvement in pain, joint motion, inflammatory markers, and disability score [5].
In noninflammatory disease, the Outerbridge classification system, originally developed for patients with chondromalacia patellae, is used (Fig. 15.2) [30]. Patients with early presentation of SLE or reactive arthritis (bacterial or viral) and those with OA with nominal radiographic changes and florid synovitis are also considered good candidates for wrist synovectomy. Patients after intra-articular fractures or multiple previous wrist interventions also benefit from capsular release, removal of adhesions, and synovectomy.
Fig. 15.2
The Outerbridge classification of articular cartilage lesions: Grade 0: Normal Cartilage, (a) Grade I: Superficial Softening, (b) Grade II: Fibrillation, (c) Grade III: Fissuring, (d) Grade IV: Loss of all Cartilage Layers and Exposure of Subchondral Bone
Arthroscopic Abrasion Chondroplasty
Chondral defects are a common source of occult pain. Fibrocartilage forms in locations of disrupted subchondral bone (Outerbridge grade IV). Abrasion and drill chondroplasty take advantage of this phenomenon and are used to fill articular defects with the goals of reducing mechanical symptoms and minimizing intra-articular debris by smoothing out the chondral lesions [9, 24, 30].
Abrasion chondroplasty is effective in patients with proximal pole hamate arthrosis, a cause of ulnar-sided wrist pain when loaded during ulnar deviation. Lunate morphology plays a key role in this condition. Patients with a type II lunate defect have a particularly positive outcome. The type II lunate and its medial facet during contact loading of the proximal pole of the hamate can lead to arthritis, with a reported occurrence in 44 % of type II lunates but only 2 % in type I lunates [11, 31–37]. In cases of advanced arthrosis and an Outerbridge grade IV lesion, we follow the recommendation of Yao and coworkers—excision of the proximal pole [31]. Abrasion arthroplasty is contraindicated for patients with active rheumatoid disease, those who are medically unfit, and patients with active infections not located in the wrist.
Also, with ulnar-sided wrist pain, it is common for patients to have concomitant injuries that also require treatment (e.g. TFCC tears, lunotriquetral interosseous ligament tears, ulnar impaction, and radial-sided pathology). When synovitis is noted on the ulnar side of the wrist, a TFCC injury is almost always noted in the absence of any other structural problem.
Arthroscopic Radial Styloidectomy
Radial styloid arthritis as a result of scapholunate advanced collapse (SLAC), scaphoid nonunion advanced collapse (SNAC), Kienböck’s disease, or impingement after scaphotrapeziotrapezoidal (STT) fusion, PRC, or four-corner fusion is the primary indication for radial styloidectomy. Arthroscopic intervention is indicated and highly effective when a PRC or fusion is not yet indicated or when patients are not ready to undergo a more extensive procedure. Arthroscopic radial styloidectomy ensures preservation of the volar ligaments, which provide radial stability of the wrist and enhance precision when determining the appropriate amount of styloid to be removed [31].
Arthroscopic Proximal Row Carpectomy
PRC has long been considered a salvage procedure of wrist arthritis because of its association with decreased range of motion, decreased strength, and progression of arthritis. Recent studies have shown its reliability to be equal to that of the four-corner fusion, which has been a well-established standard of treatment [38]. Arthroscopic PRC thus can be viewed as beneficial over the open technique because it does not require capsulotomy, does not disrupt the stabilizing ligaments, and allows for early mobilization [13]. PRC is contraindicated in the presence of arthritis at the head of the capitate or in the lunate fossa of the radius.
General Technique and Instrumentation for Arthrscopy of the Wrist
The preferred method of anesthesia in patients with arthritic changes is general or regional anesthesia. The patient is positioned supine on the operating table with the shoulder along the edge of the table. A tourniquet is placed above the elbow and inflated to 250 mmHg. The shoulder is abducted 70–90°, and finger traps from an articulating arm attached to the operating table suspend the forearm vertically. We routinely use the long and index fingers; however, all the digits may be placed in the finger traps to distribute the traction load particularly for patients with rheumatoid arthritis whose skin is delicate. A traction force of approximately 10–15 lb is applied to help open the joint and improve access during the surgical procedure (Fig. 15.3). In addition, a sling with 7–10 lb of weight is placed over the tourniquet to provide downward counter-traction and distraction of the wrist joint.
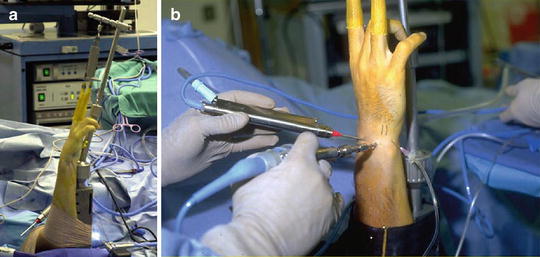
Fig. 15.3
(a) Wrist arthroscopy set up. Note the index and long fingers are placed in finger traps. 10–15 lb of traction is applied to allow for better access and mobility inside the wrist joint. (b) Wrist arthroscopy setup with instrumentation. Note arthroscope and instruments can be interchanged between portals to obtain the proper vantage point
Following patient set-up, the wrist is thoroughly examined, and relevant anatomical landmarks are palpated. The arthroscopic wrist portals are described in Table 15.1. The 3-4 portal is established in the soft spot, 1 cm distal to Lister’s tubercle (Fig. 15.4). To minimize the risk of articular cartilage damage, a 22-gauge needle is first inserted and angled 10° volar to be parallel to the radiocarpal joint surface. The wrist is then distended with 5–7 mL of saline solution. When insufflation does not occur, this sign indicates a torn TFCC. A vertical stab incision is made with a No. 15 scalpel blade through the dermis only and then a blunt trocar is introduced into the joint. To maintain orientation, the thumb is kept on Lister’s tubercle until the arthroscope is introduced. Inflow of lactated Ringer’s solution is gravity-fed (i.e. no pump required).




Table 15.1
Arthroscopic wrist portals: technique and comments
Portal | Technique | Comment |
|---|---|---|
Dorsal | ||
1-2 | Inserted in the extreme dorsum of the snuffbox just radial to the EPL tendon to avoid the radial artery. | Provides access to the radial styloid, scaphoid, lunate, and articular surface of the distal radius. |
3-4 | The portal is 1-cm distal to Lister’s tubercle between the tendons of the third and fourth compartment. | Primary working portal. Gives a wide range of movement and view. |
4-5 | Between the common extensor fourth compartment and EDQ in the fifth compartment. | Alternative to the 6R portal. |
6R | Located distal to the ulna head and radial to the ECU tendon. Established under direct vision of the arthroscope by use of a needle. Avoids damage to the TFCC. | Primary working portal. |
6U | Established under direct visualization similar to the 6R portal. Blunt dissection is always used to avoid the dorsal branches of the ulnar nerve. | 6U and 6R portals allow visualization back toward the radial side and access to the ulnar-sided structures. |
MCR | The portal is created 1-cm distal to the 3-4 portal. | Allows instrument access to the ulnar midcarpal joint. |
MCU | The portal is created 1-cm distal to the 4-5 portal. | Allows instrument access to the radial midcarpal joint. |
EPL extensor pollicis longus, EDQ extensor digiti quinti proprius, 6R 6-radial, ECU extensor carpi ulnaris, TFCC triangular fibrocartilage complex, 6U 6-ulnar, MCR mid-carpal radial, MCU mid-carpal ulnar
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
