Wrist
EPIDEMIOLOGY
The annual incidence of carpal fractures in the United States was reported at more than 678,000 in 1995.
Seven percent of distal radius fractures have an associated carpal fracture.
Carpal fractures account for 18% of all hand/wrist fractures.
Approximate incidence of carpal fractures as follows:
Scaphoid (68.2%)
Triquetrum (18.3%)
Trapezium (4.3%)
Lunate (3.9%)
Capitate (1.9%)
Hamate (1.7%)
Pisiform (1.3%)
Trapezoid (0.4%)
ANATOMY
The distal radius has articular facets for the scaphoid and lunate separated by a ridge. The sigmoid notch articulates with the distal ulna.
The distal ulna articulates with the sigmoid notch of the distal radius. The fovea (base) of the ulna styloid process serves as the attachment for the deep band of the triangular fibrocartilage complex (TFCC) while the superficial band inserts directly onto the styloid process of the ulna.
Carpal bones (Fig. 23.1)
Proximal row: This consists of the scaphoid (an oblique strut that spans both rows), lunate, triquetrum, and pisiform.
Distal row: The trapezium, trapezoid, capitate, and hamate are connected to one another and to the base of the metacarpals by strong ligaments, making the distal row relatively immobile.
The lunate is the key to carpal stability.
It is connected to both scaphoid and triquetrum by strong interosseous ligaments.
Injury to the scapholunate (SL) or lunotriquetral (LT) ligaments leads to asynchronous motion of the lunate and dissociative carpal instability patterns. SL = DISI (dorsal intercalated segmental instability) and LT tear = VISI (volar intercalated segmental instability)
The main articulations are the distal radioulnar, radiocarpal, and midcarpal.
Normal anatomic relationships (see Chapter 22)
Radial inclination: averages 23 degrees (range, 13 to 30 degrees)
Radial length: averages 11 mm (range, 8 to 18 mm)
Palmar (volar) tilt: averages 11 to 12 degrees (range, 0 to 28 degrees)
The 0-degree capitolunate angle: a straight line drawn down the third metacarpal shaft, capitate, lunate, and shaft of radius with wrist in neutral position on the lateral radiograph
The 47-degree scapholunate angle (normal range, 30 to 70 degrees); <3-mm scapholunate space
Carpal height ratio: carpal height (proximal and distal rows)/length of third metacarpal. The average is 0.53; decreased carpal height ratio indicates collapse due to carpal fracture or instability.
Wrist ligaments (Figs. 23.2 and 23.3)
Extrinsic ligaments connect the radius to the carpus and the carpus to the metacarpals.
Intrinsic ligaments connect carpal bone to carpal bone (e.g., scapholunate and lunotriquetral ligaments).
The thickest and strongest region of the scapholunate ligament is located dorsally while that of the lunotriquetral ligament is located palmarly.
Important volar ligaments include:
The radioscaphocapitate, which acts as a fulcrum around which the scaphoid rotates and guides scaphoid kinematics
The radioscapholunate, also called the ligament of Testut (not a strong ligament, it is a neurovascular tuft of synovium derived from the anterior interosseous and radial arteries as well as the anterior interosseous nerve)
The short radiolunate which is contiguous with the palmar fibres of the TFCC
The radiolunotriquetral (supports the proximal row, stabilizes the radiolunate and lunotriquetral joints)
The important dorsal ligaments are:
The dorsal intercarpal, which originate from the triquetrum and extend radially to insert onto the lunate, the dorsal groove of the scaphoid, and the trapezium
The radiocarpal, which originate from the dorsal margin of the distal radius and attach to the lunate and triquetrum.
The proximal and distal carpal rows are attached by capsular ligaments on each side of the lunocapitate joint.
Injury to these extrinsic ligaments leads to abnormal motion between the two rows and to nondissociative wrist instability patterns.
Space of Poirier: This is a ligament-free area situated between the radioscaphocapitate ligament and the long radiolunate ligament at the level of the midcarpal joint, which is an area of potential weakness.
The TFCC is a major stabilizer of the ulnar carpus and distal radioulnar joint.
The TFCC stabilizes the distal radial ulnar joint (DRUJ) and absorbs about 20% of the axial load across the wrist joint at neutral ulnar variance.
It consists of several components, including the dorsal and volar radioulnar ligaments, articular disc, meniscal homologue, extensor carpi ulnaris subsheath, and origins of the ulnolunate and ulnotriquetral ligaments.
Vascular supply (Fig. 23.4)
The radial, ulnar, and anterior interosseous arteries combine to form a network of transverse arterial arches both dorsal and volar to the carpus.
The blood supply to the scaphoid is derived primarily from the radial artery, both dorsally and volarly. The volar scaphoid branches supply the distal 20% to 30% of the scaphoid, whereas branches entering the dorsal ridge supply the proximal 70% to 80%, via interosseous blood supply, similar to the femoral head.
The lunate receives blood supply from both its volar and dorsal surfaces in most cases (80%). About 20% of lunates have only a volar blood supply.
Kinematics
The global motion of the wrist is composed of flexion and extension, radioulnar deviation at the radiocarpal joint, and axial rotation around the DRUJ.
The radiocarpal articulation acts as a universal joint, allowing a small degree of intercarpal motion related to rotation of individual carpal bones.
The forearm accounts for about 140 degrees of rotation.
Radiocarpal joint motion is primarily flexion and extension of nearly equal proportions (70 degrees), and radial and ulnar deviation of 20 and 40 degrees, respectively.
The scaphoid rests on the radioscaphocapitate ligament at its waist. Using the ligament as an axis, it rotates from a volar flexed perpendicular position to a dorsiflexed longitudinal position. With the wrist in radial deviation, the scaphoid flexes; with ulnar deviation, the scaphoid extends.
Pathomechanics (Fig. 23.5)
Classically, the radius, lunate, and capitate have been described as a central “link” that is colinear in the sagittal plane.
The scaphoid serves as a connecting strut. Any flexion moment transmitted across the scaphoid is balanced by an extension moment at the triquetrum.
When the scaphoid is destabilized by fracture or scapholunate ligament disruption, the lunate and triquetrum assume a position of excessive dorsiflexion (dorsal intercalated segmental instability [DISI]) and the scapholunate angle becomes abnormally high (>70 degrees).
When the triquetrum is destabilized (usually by disruption of the lunotriquetral ligament complex), the opposite pattern (volar intercalated segmental instability [VISI]) is seen as the lunate (intercalated segment) volar flexes.
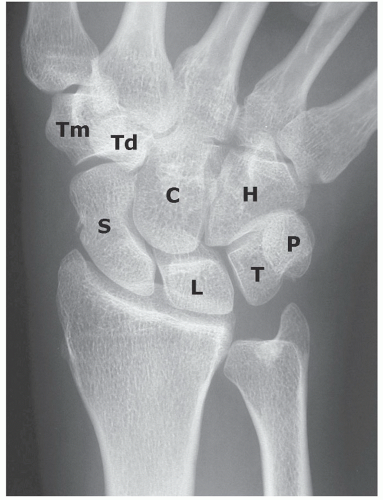 FIGURE 23.1 The wrist is composed of two rows of bones that provide motion and transfer forces: scaphoid (S ), lunate (L), triquetrum (T), pisiform (P), trapezium (Tm), trapezoid (Td), capitate (C ), hamate (H ). (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
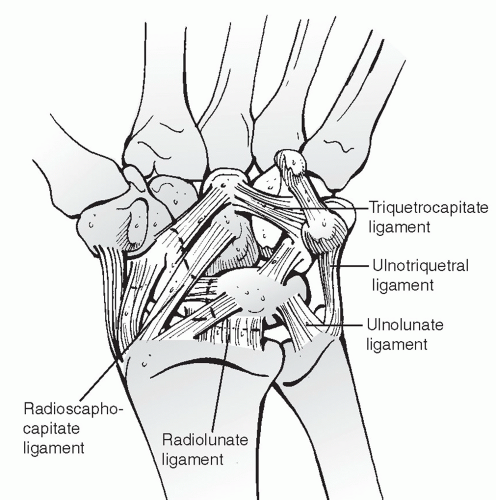 FIGURE 23.2 The palmar capsule consists of two major ligamentous inclusions: the radiolunate ligament is the deeper of the two, which proceeds to the triquetrum and composes in effect the radiolunotriquetral ligament. The more distal and superficial component is often referred to as the arcuate ligament or distal V. The radial component of this ligament is the radioscaphocapitate ligament. The ulnar component of the arcuate ligament is the triquetrocapitate ligament. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
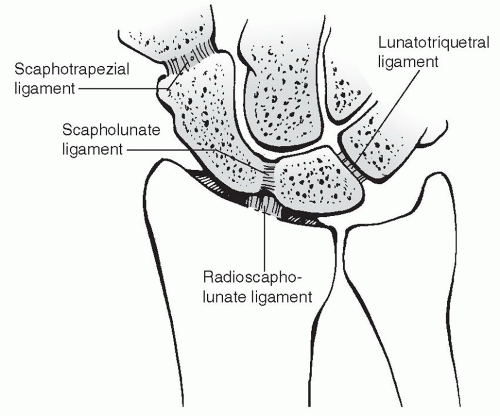 FIGURE 23.3 The intra-articular intrinsic ligaments connect adjacent carpal bones. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
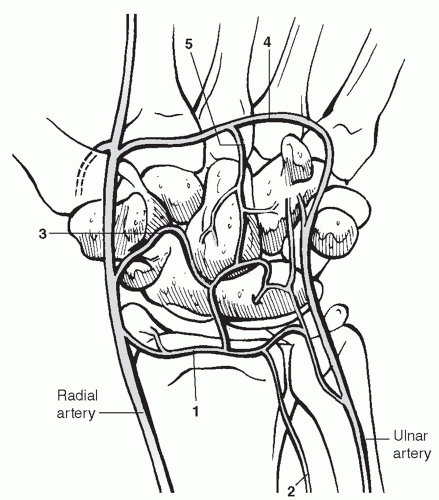 FIGURE 23.4 Schematic drawing of the arterial supply of the palmar aspect of the carpus. Circulation of the wrist is obtained through the radial, ulnar, and anterior interosseous arteries and the deep palmar arch: 1, palmar radiocarpal arch; 2, palmar branch of anterior interosseous artery; 3, palmar intercarpal arch; 4, deep palmar arch; and 5, recurrent artery. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
MECHANISM OF INJURY
The most common mechanism of carpal injury is a fall onto the outstretched hand, resulting in an axial compressive force with the wrist in hyperextension. The volar ligaments are placed under tension with compression and shear forces applied dorsally, especially when the wrist is extended beyond its physiologic limits.
Excessive ulnar deviation and intercarpal supination result in a predictable pattern of perilunate injury, progressing from the radial side of the carpus to the midcarpus and finally to the ulnar carpus.
Direct mechanisms of injury such as crush injuries should alert the clinician to the possible development of compartment syndrome of the hand.
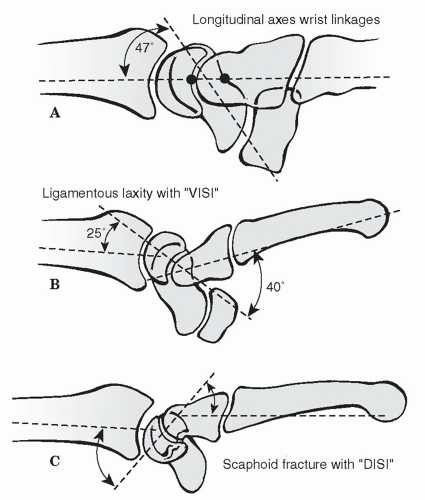 FIGURE 23.5 Schematic drawing of carpal instability. (A) Normal longitudinal alignment of the carpal bones with the scaphoid axis at a 47-degree angle to the axes of the capitate, lunate, and radius. (B) A volar intercalated segmental instability (VISI) deformity is usually associated with disruption of the lunotriquetral ligament. (C) A dorsal intercalated segmental instability (DISI) deformity is associated with scapholunate ligament disruption or a displaced scaphoid fracture. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Baltimore: Lippincott Williams & Wilkins; 2005.) |
CLINICAL EVALUATION
The clinical presentation of individual carpal injuries is variable, but in general, the most consistent sign of carpal injury is well-localized tenderness.
Gross deformity may be present, ranging from displacement of the carpus to prominence of individual carpal bones.
A complete evaluation of the median, radial, ulnar, and digital nerves is warranted as well as assessment of capillary refill, color, and temperature.
Provocative tests may reproduce or exacerbate pain, crepitus, or displacement indicative of individual carpal injuries (see specific carpal injuries).
RADIOGRAPHIC EVALUATION
Posteroanterior (PA), oblique, and lateral x-rays are each taken with the wrist in the neutral position.
Gilula lines (three smooth radiographic arcs) should be examined on the PA view. Disruption of these arcs indicates ligamentous instability.
For further diagnosis of carpal and mainly scaphoid fractures:
A scaphoid view (anteroposterior [AP] x-ray with wrist supinated 30 degrees and in ulnar deviation) is obtained.
A pronated oblique view is indicated.
If there is the suspicion of carpal instability, additional views in maximal radial and ulnar deviation are recommended as well as bilateral clenched-fist PA to look for widening of the scapholunate interval.
Further views can be done in maximal flexion and extension.
Arthrography, magnetic resonance (MR), wrist arthrography, videoradiography, and arthroscopy can assist in the diagnosis of carpal ligament injuries.
Computed tomography (CT) scans are helpful in evaluating carpal fractures, malunion, nonunion, and bone loss.
Magnetic resonance imaging (MRI) scans are sensitive to detect occult fractures and osteonecrosis of the carpal bones as well as detecting soft tissue injury, including ruptures of the scapholunate ligament and TFCC.
CLASSIFICATION
Orthopaedic Trauma Association Classification of Carpal Fractures and Fracture-Dislocations
See Fracture and Dislocation Compendium at http://ota.org/.compendium/index.htm.
SPECIFIC FRACTURES
Scaphoid
Fractures of the scaphoid are common and account for about 50% to 80% of carpal injuries.
About 345,000 scaphoid fractures occur annually in the United States and account for 1 in every 100,000 emergency room visits.
Anatomically, the scaphoid is divided into proximal and distal poles, a tubercle, and a waist; 80% of the scaphoid is covered with articular cartilage (Fig. 23.6).
Eighty percent of scaphoid fractures occur at its waist, 10% to 20% involve the proximal pole, and 5% occur at its distal pole and tuberosity.
Ligamentous attachments to the scaphoid include the radioscaphocapitate ligament, which variably attaches to the ulnar aspect of the scaphoid waist, and the dorsal intercarpal ligament, which provides the primary vascular supply to the scaphoid.
The major vascular supply is derived from scaphoid branches of the radial artery, entering the dorsal ridge and supplying 70% to 80% of the scaphoid, including the proximal pole. The remaining distal aspect is supplied through branches entering the tubercle. Fractures at the scaphoid waist or proximal third depend on fracture union for revascularization (Fig. 23.7).
The most common mechanism is a fall onto the outstretched hand that imposes a force of dorsiflexion, ulnar deviation, and intercarpal supination.
Clinical evaluation:Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



