General Spine
EPIDEMIOLOGY
There are approximately 12,000 new spinal cord injuries requiring treatment each year.
Injury to the vertebral column occurs much less frequently than injury to the appendicular skeleton, and vertebral column fractures account for approximately 6% of all fractures.
Fifteen percent to 20% of vertebral fractures can occur at multiple noncontiguous levels.
Motor vehicle accidents account for approximately 50% of all traumatic spinal cord injuries.
In patients with spinal cord injury, the overall mortality during the initial hospitalization is 17%.
Approximately 2% to 6% of trauma patients sustain a cervical spine fracture.
The ratio of male to female patients sustaining vertebral fractures is 4:1.
The lifetime direct medical cost of spinal cord injury for persons injured at age 25 years is estimated to be between $1.5 and $4.6 million depending on injury severity.
ANATOMY
The spinal cord occupies approximately 35% of the canal at the level of the atlas (C1) and 50% of the canal in the lower cervical spine and thoracolumbar segments. The remainder of the canal is filled with epidural fat, cerebrospinal fluid, and dura mater.
The conus medullaris represents the caudal termination of the spinal cord. It contains the sacral and coccygeal myelomeres and lies dorsal to the L1 body and L1-L2 intervertebral disc.
The cauda equina (literally translated means “horse’s tail”) represents the motor and sensory roots of the lumbosacral myelomeres. These roots are less likely to be injured because they have more room in the canal and are not tethered to the same degree as the spinal cord.
Furthermore, the motor nerve roots are composed of lower motor neurons, which are more resilient to injury than the upper motor neurons of the brain and spinal cord.
A reflex arc is a simple sensorimotor pathway that can function without using either ascending or descending white matter long tract axons. A spinal cord level that is anatomically and physiologically intact may demonstrate a functional reflex arc at that level despite dysfunction of the spinal cord cephalad to that level.
MECHANISM OF INJURY
A long-standing and fundamental problem of classifying spinal injury based on presumed mechanism of injury is that the same mechanism of injury can result in morphologically different patterns of injury; similar morphologic patterns of injury can also be the result of different injury mechanisms, and the patterns of head deflection do not predict spinal injury patterns. Several characteristics of the injury force that determine the extent of neural tissue damage have been identified. These include the rate of force application, the degree of neural tissue compression, and the duration of neural tissue compression.
Primary Injury
Primary injury refers to physical tissue disruption caused by mechanical forces.
Contusion: This sudden, brief compression by a displaced structure affects central tissues primarily and accounts for the majority of primary injuries; thus, it is responsible for the majority of neurologic deficits. Contusion injuries are potentially reversible, although irreversible neuronal death occurs along with vascular injury and intramedullary hemorrhage.
Compression: Injury results from decreased size of the spinal canal; it may occur with translation or angulation of the spinal column, as in burst injuries or epidural hematomas. Injury occurs by:
Mechanical deformation interrupting axonal flow
Interruption of spinal vascularity resulting in ischemia of neurologic structures
Stretch: Injury results in longitudinal traction, as in the case of a flexion-distraction injury. Injury occurs as a result of capillary and axonal collapse secondary to tensile distortion.
Laceration: This is caused by penetrating foreign bodies, missile fragments, or displaced bone.
Secondary Injury
Secondary injury refers to additional neural tissue damage resulting from the biologic response initiated by physical tissue disruption.
Local tissue elements undergo structural and chemical changes. These changes, in turn, elicit systemic responses. Changes in local blood flow, tissue edema, metabolite concentrations, and concentrations of chemical mediators lead to propagation of interdependent reactions. This pathophysiologic response, referred to as secondary injury, can propagate tissue destruction and functional loss.
Local tissue elements undergo structural and chemical changes. These changes, in turn, elicit systemic responses. Changes in local blood flow, tissue edema, metabolite concentrations, and concentrations of chemical mediators lead to propagation of interdependent reactions. This pathophysiologic response, referred to as secondary injury, can propagate tissue destruction and functional loss.
CLINICAL EVALUATION
Assess the patient: Airway, breathing, circulation, disability, and exposure (ABCDE). Avoid the head-tilt-chin-lift maneuver, hypoxia, and hypotension.
Initiate resuscitation: Address life-threatening injuries.
Evaluate the patient’s level of consciousness.
Evaluate injuries to the head, chest, abdomen, pelvis, and spine.
The spine should be protected at all times during the management of a multiply injured patient. The ideal position is with the whole spine immobilized in a neutral position on a firm surface. This may be achieved manually or with a combination of semirigid cervical collars, side head supports, and strapping. Strapping should be applied to the shoulders and pelvis as well as the head to prevent the neck becoming the center of rotation of the body.
Take extreme care when logrolling the patient to assess the spinal column, as there is significant risk of injuring the spinal cord if there is instability. Examine the skin for bruising and abrasions, and palpate spinous processes for tenderness and diastasis. The patient should be placed on a scoop stretcher or long spine board with the head and neck supported.
Calenoff found a 5% incidence of multiple noncontiguous vertebral injuries. Half of the secondary lesions were initially missed, with a mean delay of 53 days in diagnosis; 40% of secondary lesions occurred above the primary lesion and 60% below. The region T2 through T7 accounted for 47% of primary lesions in this population but only 16% of reported spinal injuries in general.
Injuries of the vertebral column tend to cluster at the junctional areas: the craniocervical junction (occiput to C2), the cervicothoracic junction (C7-T1), and the thoracolumbar junction (T11-L2). These areas represent regions of stress concentration, where a rigid segment of the spine meets a more flexible segment. Also contributing to stress concentration in these regions are changes at these levels in the movement constraints of vertebrae.
Among these injuries, the most serious and most frequently missed is craniocervical dissociation.
In trauma patients, thoracic and lumbar fractures are concentrated at the thoracolumbar junction, with 60% of thoracic and lumbar fractures occurring between T11 and L2 vertebral levels.
Three common patterns of noncontiguous spinal injuries are as follows.
Assess injuries to the extremities.
Complete the neurologic examination to evaluate reflexes, sensation (touch, pain), and motor function (Fig. 8.1 and Table 8.1).
Perform a rectal examination to test for perianal sensation, resting tone, and the bulbocavernosus reflex.
Pattern A: Primary injury at C5-C7, with secondary injuries at T12 or in the lumbar spine
Pattern B: Primary injury at T2-T4, with secondary injuries in the cervical spine
Pattern C: Primary injury at T12-L2, with a secondary injury at L4-L5
Spinal Shock
Spinal shock is defined as spinal cord dysfunction based on physiologic rather than structural disruption. Resolution of spinal shock may be recognized when reflex arcs caudal to the level of injury begin to function again, usually within 24 hours of injury.
Spinal shock should be distinguished from neurogenic shock, which refers to hypotension associated with loss of peripheral vascular resistance in spinal cord injury.
Neurogenic Shock
Neurogenic shock (Table 8.2) refers to flaccid paralysis, areflexia, and lack of sensation to physiologic spinal cord “shutdown” in response to injury.
It is most common in cervical and upper thoracic injuries.
It almost always resolves within 24 to 48 hours.
The bulbocavernosus reflex (S3-S4) is the first to return (Table 8.3).
Initial tachycardia and hypertension immediately after injury are followed by hypotension accompanied by bradycardia and venous pooling.
Hypotension from neurogenic shock may be differentiated from cardiogenic, septic, and hypovolemic shock by the presence of associated bradycardia, as opposed to tachycardia.
Treatment is based on administration of isotonic fluids, with careful assessment of fluid status (beware of overhydration).
Recognizing neurogenic shock as distinct from hemorrhagic shock is critical for safe initial resuscitation of a trauma patient. Treatment of neurogenic shock is pharmacologic intervention to augment peripheral vascular tone. This vascular tone may be essential for effective resuscitation. Fluid overload from excessive fluid volume administration, typical in treatment of hemorrhagic shock, can result in pulmonary edema in the setting of neurogenic shock.
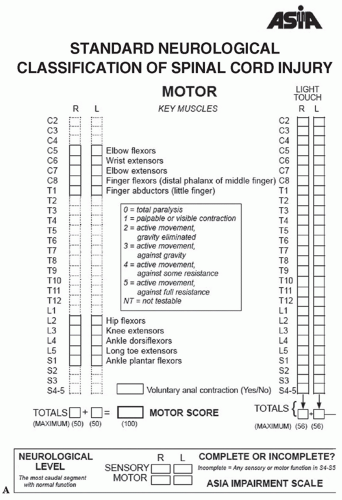 FIGURE 8.1 Neurologic examination recommended by the American Spinal Injury Association (ASIA). (A) Motor score and (B) sensory score. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
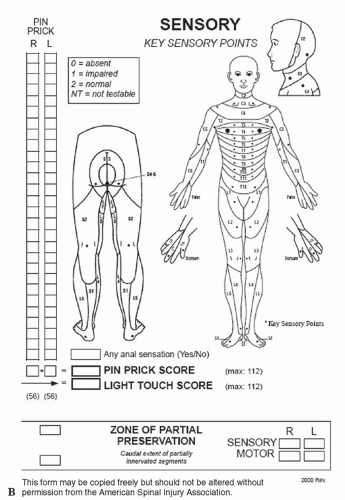 FIGURE 8.1 (Continued) |
Bulbocavernosus Reflex
The bulbocavernosus reflex refers to contraction of the anal sphincter in response to a squeeze on the glans penis in a male, the clitoris or the mons pubis in a female, or a pull on the urethral catheter.
The absence of this reflex indicates spinal shock.
The return of the bulbocavernosus reflex heralds the end of spinal shock and generally occurs within 24 hours of the initial injury.
The presence of a complete lesion after spinal shock has resolved portends a virtually nonexistent chance of neurologic recovery.
The bulbocavernosus reflex is not prognostic for lesions involving the conus medullaris or the cauda equina.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


