Distal Radius
EPIDEMIOLOGY
Distal radius fractures are among the most common fractures of the upper extremity.
More than 650,000 occur annually in the United States.
Fractures of the distal radius represent approximately one-sixth of all fractures treated in emergency departments and about 16% of all fractures treated by orthopaedic surgeons.
The incidence of distal radius fractures in the elderly correlates with osteopenia and rises in incidence with increasing age, nearly in parallel with the increased incidence of hip fractures.
In men aged 35 years and older, the incidence is approximately 90 per 100,000 population per year and remains relatively constant until the age of 70 where a slight increase is seen.
In women less than age 40, the incidence is approximately 368 per 100,000 population; for women 40 years and older, this incidence rises to 1,150 per 100,000 population.
Risk factors for fractures of the distal radius in the elderly include decreased bone mineral density, female sex, white race, family history, and early menopause.
ANATOMY
The metaphysis of the distal radius is composed primarily of cancellous bone. The articular surface has a biconcave surface for articulation with the proximal carpal row (scaphoid and lunate fossae), as well as a notch for articulation with the distal ulna.
Eighty percent of axial load is supported by the distal radius and 20% by the ulna and the triangular fibrocartilage complex (TFCC).
Reversal of the normal palmar tilt results in load transfer onto the ulna and TFCC; the remaining load is then borne eccentrically by the distal radius and is concentrated on the dorsal aspect of the scaphoid fossa.
Numerous ligamentous attachments exist to the distal radius; these often remain intact during distal radius fracture, facilitating reduction through “ligamentotaxis.”
The volar ligaments are stronger and confer more stability to the radiocarpal articulation than the dorsal ligaments.
MECHANISM OF INJURY
Common mechanisms in younger individuals include falls from a height, motor vehicle accidents, or injuries sustained during athletic participation. In elderly individuals, distal radial fractures may arise from low-energy mechanisms, such as a simple fall from a standing height, and as such are considered a fragility fracture.
The most common mechanism of injury is a fall onto an outstretched hand with the wrist in dorsiflexion.
Fractures of the distal radius are produced when the dorsiflexion of the wrist varies between 40 and 90 degrees.
The radius initially fails in tension on the volar aspect, with the fracture propagating dorsally, whereas bending moment forces induce compression stresses, resulting in dorsal comminution. Cancellous impaction of the metaphysis further compromises dorsal stability. Additionally, shearing forces influence the injury pattern, often resulting in articular surface involvement.
High-energy injuries (e.g., vehicular trauma) may result in significantly displaced or highly comminuted unstable fractures to the distal radius.
CLINICAL EVALUATION
Patients typically present with variable wrist deformity and displacement of the hand in relation to the wrist (dorsal in Colles or dorsal Barton fractures and volar in Smith-type fractures or volar Bartons). The wrist is typically swollen with ecchymosis, tenderness, and painful range of motion.
The ipsilateral elbow and shoulder should be examined for associated injuries.
A careful neurovascular assessment should be performed, with particular attention to median nerve function. Carpal tunnel compression symptoms are common (13% to 23%) owing to traction during forced hyperextension of the wrist, direct trauma from fracture fragments, hematoma formation, or increased compartment pressure.
RADIOGRAPHIC EVALUATION
Posteroanterior and lateral views of the wrist should be obtained, with oblique views for further fracture definition, if necessary. Shoulder or elbow symptoms should be evaluated radiographically.
Contralateral wrist views may help to assess the patient’s normal ulnar variance and scapholunate angle.
Computed tomography scan may help to demonstrate the extent of intra-articular involvement.
Normal radiographic relationships (Fig. 22.1):
Radial inclination: averages 23 degrees (range, 13 to 30 degrees)
Radial length: averages 11 mm (range, 8 to 18 mm)
Palmar (volar) tilt: averages 11 to 12 degrees (range, 0 to 28 degrees)
CLASSIFICATION
Descriptive
Open versus closed
Displacement
Angulation
Comminution
Loss of radial length
Frykman Classification of Colles Fractures
This is based on the pattern of intra-articular involvement (Fig. 22.2).
| ||||||||||||||||||
Fernandez Classification
This is a mechanism-based classification system.
Type I: Metaphyseal bending fracture with the inherent problems of loss of palmar tilt and radial shortening relative to the ulna (DRUJ injury)
Type II: Shearing fracture requiring reduction and often buttressing of the articular segment
Type III: Compression of the articular surface without the characteristic fragmentation; also the potential for significant interosseous ligament injury
Type IV: Avulsion fracture or radiocarpal fracture-dislocation
Type V: Combined injury with significant soft tissue involvement owing to high-energy injury
 FIGURE 22.1 (A-C) The normal radiographic measurements of the distal radius. (Reproduced with permission from the Orthopaedic Trauma Association.) |
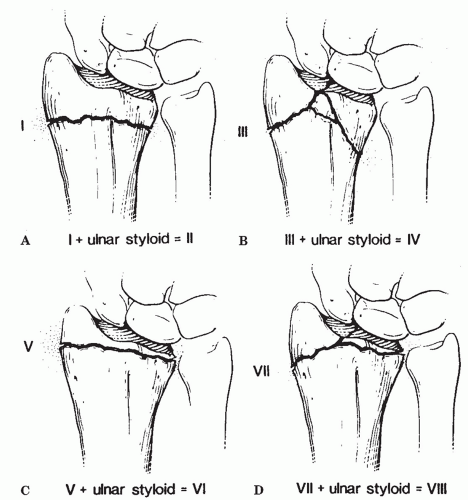 FIGURE 22.2 Frykman classification of distal radius fractures. (A) Frykman type I/II, extra-articular. (B) Frykman type III/IV, intra-articular radiocarpal joint. (C) Frykman type V/VI, intra-articular distal radioulnar joint. (D) Frykman type VII/VIII, intra-articular radiocarpal and distal radioulnar joints. (From Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults. Vol 1. 4th ed. Philadelphia: Lippincott-Raven; 1996:771.) |
Orthopaedic Trauma Association Classification of Fractures of the Distal Radius and Ulna
See Fracture and Dislocation Compendium at http://www.ota.org/compendium/index.htm.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


