Abstract
Objective
The aim of this study was to adapt and validate the Tunisian version of the Oswestry Disability Index (ODI) within a Saudi Arabian population.
Method
The translation of items 8 and 10 taken out of the Tunisian version was conducted according to Beaton’s method. Adaptations were made after a pilot study on 100 patients. The validation study included 100 patients suffering from chronic low back pain aged 18 to 65 years old. Intra-observer reliability was assessed using the intra-class coefficient (ICC). Spearman rank correlation coefficient, the Kruskall–Wallis test and factor analysis were used to evaluate construct validity (convergent and divergent validity). Internal consistency was assessed by Cronbach’s alpha coefficient.
Results
One hundred Saudi patients were included in the study. Intra-observer reliability was excellent (ICC: 0.99). The correlations of the index with the VAS pain scale ( r = 0.708), the Roland–Morris Low Back Pain Disability ( r = 0.656), and the Quebec Back Pain Disability Scale ( r = 0.792) suggest good construct validity. Factor analysis unveiled two main factors explaining a cumulative percentage variance of 63.5%. The first factor represents static activities and the second factor represents dynamic activities.
Conclusion
The Arabic version of the ODI adapted to the Saudi population has high metrological qualities. Further studies assessing its responsiveness to change should be conducted.
Résumé
Objectif
Adapter et valider la version tunisienne de l’indice fonctionnel d’Oswestry (ODI) pour lombalgie sur une population saoudienne.
Patients et méthodes
La traduction des items 8 et 10 retirés de la version tunisienne a été faite selon la méthode de Beaton. Des adaptations ont été faites après pré-test sur 100 sujets. La validation a inclus une série de 100 patients lombalgiques chroniques âgés entre 18 et 65 ans. La reproductibilité a été jugée par le coefficient de corrélation intra-classe (CCI). La validité de construit (validités de divergence et de convergence) a été évaluée à l’aide du coefficient de Spearman, du test de Kruskall–Wallis, et d’une analyse factorielle suivie d’une rotation orthogonale. La cohérence interne a été faite à l’aide du coefficient de Crohnbach.
Résultats
Cent patients saoudiens ont participé à l’étude. La reproductibilité était excellente (CCI : 0,99). Les corrélations de l’indice d’Oswestry avec l’EVA douleur ( r = 0,708), avec le Roland–Morris Low Back Pain Disability ( r = 0,656) et le Québec Back Pain Disability Scale ( r = 0,792) lui confère une bonne validité de construit. L’analyse factorielle a permis d’extraire deux facteurs expliquant 63,5 % de la variance totale. Le premier représente les activités statiques et le deuxième les activités dynamiques.
Conclusion
La version arabe adaptée à la population saoudienne a des qualités métrologiques satisfaisantes. Des études explorant la sensibilité au changement doivent être menées.
1
English version
1.1
Introduction
Nowadays, low back pain has become a real public health issue in industrialized and developing countries alike . The annual cost for the care management of patients with low back pain is estimated at more than 50 billion dollars in the United States, and 6.1 millions of Swiss Francs in Switzerland . In Saudi Arabia, the prevalence of low back pain has not been properly established, but it is estimated at 26.2% .
It is a benign affection, resolving spontaneously in most cases . It preferentially affects active young adults. Even though, the clinical examination is important in evaluating patients, it cannot assess the impact of the disease on the patient’s functional status .
Several scales have been developed for the functional evaluation of patients with low back pain, very few of them were validated .
Among these scales, we can find the Roland–Morris Disability Questionnaire , the Dallas Pain Questionnaire , the Quebec Back Pain Disability Scale , the Waddell Disability Index , the Million Visual Analog Scale , the Low Back outcome score and the Oswestry Low Back Pain Disability Questionnaire (ODI) . The latter being one of the most used scales in the literature worldwide. It was created in the 1980s with different adaptations published over the years to reach its final version 2.1 .
This index was validated in different languages including Arabic validated on a Tunisian population . This offers the possibility of conducting comparative studies in the different regions of the world. However, no index has been validated in Saudi Arabia.
The objective of our work was to study the metrological properties of the Tunisian Arabic version of the ODI on a Saudi population of patients with low back pain.
1.2
Materials and methods
1.2.1
The index
The Oswestry Low Back Pain Disability Index ( Appendix A ) is a 10-item self-assessing questionnaire, each item contains 6 levels of answers that can be scored from 0 to 5. These items are: pain, personal care, lifting and moving objects, walking, sitting, standing, sleep disorders caused by the low back pain, sex life, social life, and traveling. A total score is calculated, percentage of disability (score obtained divided by 50 and multiplied by 100) ranges from 0% (no disability) to 100% (complete disability). The interpretation of this scale is based on the scores: from 0 to 20%: minimal disability; from 20 to 40% moderate disability; from 40 to 60%: severe disability; from 60 to 80% crippling low back pain and beyond 80% the person is confined to bed, i.e. excessive incapacity .
1.2.2
Adapting the questionnaire
We started with the validated Tunisian version . A translation in Arabic (close to the dialect) was conducted according to the translation/back translation method for the items missing in the Tunisian version (items 8 and 10) . The intermediate and definite versions were submitted to an experts’ committee made of 4 linguistic professionals, 2 physiotherapists and 1 Physical Medicine and Rehabilitation physician to bring the necessary adaptations on a linguistic and cultural level.
1.2.3
Pre-test
The translated questionnaire was tested on a group of 100 healthy volunteers from the general population (pre-test). In order to verify its acceptability, we evaluated the comprehension of the questions and number of missing answers. These persons came from 10 different regions of the kingdom of Saudi Arabia (Riyadh, Assir, Bisha, Mecca, Al-Medina, Qassim, Araar, Hafr El-Baten, Dammam and Jeddah).
Twenty volunteer physiotherapists (10 men and 10 women), 2 per region (one man and one woman) were in charge of the pre-test. The choice of the regions was based on geographic and linguistic characteristics of the kingdom. Only the persons speaking Arabic were included in the study. At the end of this step, we obtained an intermediate scale.
1.2.4
Cohort study
1.2.4.1
Patients
Were included in this study, patients aged 18 to 65 referred to the rehabilitation department for chronic mechanical low back pain.
Clinical and demographic data were collected for all patients during the first consultation. Only patients who were clinically stable were chosen for the reproducibility study.
Questions were enunciated out loud word for word exactly as they were written. The investigator could not change the words but had the possibility to repeat the questions. The levels of comprehension and acceptability were noted for each question.
1.2.5
Evaluation of the metrological properties of the final version
1.2.5.1
Feasibility and acceptability
The feasibility and acceptability of the scale were appreciated by the number of missing data for each item, the comprehension of the questions asked and the time required to complete the questionnaire.
1.2.5.2
Reproducibility study
The questionnaire was administered twice to 50 patients by the same investigator at a 2-day interval. The choice of this interval was based on the need for a stable clinical status on the one hand and patients not memorizing the answers on the other hand (time needed to fill-out the questionnaire, missing answers).
1.2.5.3
Validity study
1.2.5.3.1
Appearance validity
The appearance validity study was based both on the appreciation of the experts’ committee and the judgment of users.
1.2.5.3.2
Content validity
The content validity study was based on the appreciation of the experts’ committee. According to their experience, the experts evaluated the quality of the scale’s items by comparing the translated scale to the original one.
1.2.5.3.3
Construct validity
In the absence of a “Gold Standard”, the assessment of the questionnaire’s factor structure was based on construct validity, which includes convergent and divergent validity, as well as evaluating the validity of the factor structure.
Convergent validity was evaluated by correlating the global score of the ODI to the scores of similar scales measuring functional impairments and/or pain. The scales used were: Pain Visual Analog Scale (VAS), the score of the Roland–Morris Low Back Pain Disability Questionnaire and the score of the Quebec Back Pain Disability Scale.
Divergent validity was assessed by studying the correlation of ODI’s global score to variables known for having null or minimal relationships with pain or functional impairments. These selected variables were: age, weight height, and educational level.
A factor analysis followed by a Varimax rotation allowed us to study the factor structure validity of the scale. The internal consistency of the scale and each factor extracted after the factor analysis were studied by the Cronbach’s alpha coefficient.
1.2.6
Statistical analysis
We used the SPSS software for Windows (version 14) to conduct the statistical analysis with a significant threshold set at P < 0.05.
Quantitative variables were described using means, standard deviations and limits. Qualitative variables were described using proportions and percentages.
Reproducibility was assessed through the intra-class correlation coefficient (ICC) item per item and for the global score. A good reproducibility was noted when ICC > 0.7 .
Convergent and discriminating validities were studied with Kruskall–Wallis test for discontinued variables and the Spearman’s rank correlation coefficient for continuous variables. For the latter, based on the value of the coefficient and according to Fermanian, the results were deemed excellent if r > 0.91, good if 0.71 < r < 0.9, moderate if 0.51 < r <0.7, poor if 0.31; 1; < r < 0.5, very poor or null if r < 0.3 .
The factor analysis was conducted using main components to extract the main factors. The identified factors had a value > 1. Independent factors were obtained using the Varimax rotation. The internal consistency of each of these identified factors was assessed with the Cronbach’s alpha test. A coefficient > 0.7 reflected a good internal consistency.
1.3
Results
1.3.1
The intermediate scale and pre-test
For items 8 and 10, the translation/back translation technique led to linguistic adaptations, focusing on promoting the meaning of the item rather than achieving a literal translation.
This step gave way to some linguistic changes of the different items of the scale: terms that seemed difficult to understand for the patients were replaced by other more simple ones while keeping the meaning of the questions.
The main changes concerned semantic and syntax issues.
Thus, the terms“Awjaa” and“Wajaa” used in the Tunisian version were replaced respectively by “Aalam” and “Alam” closer to the Saudi culture, these terms, in literary Arabic, mean pain and complaint. Furthermore, the adjective “lumbar” was added to the term pain for all items.
The intermediate version of our index was the object of a study and completed by 100 healthy volunteers (50 women and 50 men), mean age 39.7 years (min 18; max 65) including 19 illiterate subjects.
After the pre-test, neither the number of items nor the answer modalities were altered.
1.3.2
Clinical and demographic data for the series
In the final study, 100 patients were included, 45% were female, mean age was 40.39 ± 12.70 years, mean weight was 75.64 ± 16.03 kg, mean height was 164.96 ± 9.15 mm. Only 12% of the subjects were unemployed at the time of the study.
The repartition of subjects according to educational level was the following: primary school: 11; middle school: 12; high school: 24; university: 42; and illiterate subjects: 11.
1.3.3
Changes made to the intermediate scale
After studying the series, no changes were made to the intermediate scale and no items were taken out.
1.3.4
Metrological properties of the index
1.3.4.1
Feasibility and acceptability
The mean time required to complete the questionnaire was 3.4 minutes (min 2; max 6).
Acceptability was good for all items.
1.3.4.2
Reproducibility
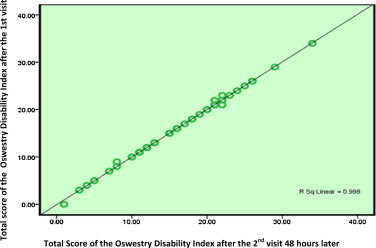
ICC was 0.999 (CI at 95%: 0.998–0.999). Intra-observer reproducibility was excellent ( Fig. 1 ). Item per item reproducibility showed a correlation coefficient ranging from 0.75 to 0.99 ( Table 1 ).
| Item | Intra-class correlation coefficient |
|---|---|
| 1 | 0.82 |
| 2 | 0.73 |
| 3 | 0.99 |
| 4 | 0.84 |
| 5 | 0.80 |
| 6 | 0.99 |
| 7 | 0.92 |
| 8 | 0.92 |
| 9 | 0.90 |
| 10 | 0.88 |
| Global score | 0.99 |
1.3.5
Validity
1.3.5.1
Appearance validity
The translated version of the index included the same number of items as the original index, thus, its appearance validity can be extrapolated from the original index and therefore our scale exhibits good appearance validity.
1.3.5.2
Content validity
Our scale had a satisfying homogeneity between the various dimensions. This good internal consistency was validated by Cronbach’s alpha coefficient calculated at 0.886.
1.3.5.3
Structure validity
1.3.5.3.1
Construct validity
* No significant correlation was found for the discriminating criteria, i.e. age ( r = 0.268), weight ( r = 0.112), height ( r = –0.062), and educational level ( P = 0.112). The index has good divergent validity.
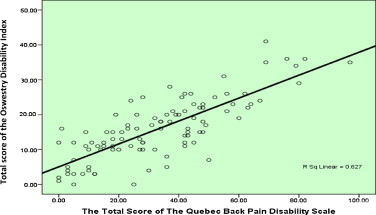
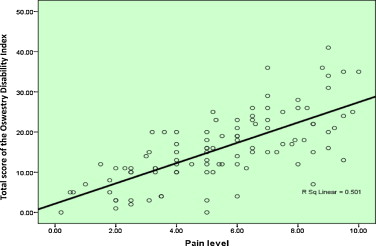
* The correlations of our index with the pain VAS ( r = 0.708, P < 0.01), the Quebec Back Pain Disability Scale ( r = 0.792, P < 0.01), and the Roland–Morris Low Back Pain Disability ( r = 0,656, P < 0.01) were deemed satisfactory. The ODI has a good convergent validity ( Figs. 2–4 and Table 2 ).

| Correlation with the Oswestry Index (Spearman r ) | P | |
|---|---|---|
| Convergent criteria | ||
| Pain VAS | 0.708 | < 0.001 |
| Roland–Morris questionnaire | 0.656 | < 0.001 |
| Quebec Scale | 0.792 | < 0.001 |
| Discriminating criteria | ||
| Age | 0.268 | 0.01 |
| Weight | 0.112 | 0.01 |
| Height | –0.062 | 0.01 |
| Education | Correlation studied with Kruskall–Wallis | 0.112 |
1.3.5.3.2
Internal structure validity
The principal component factor analysis of the ODI allowed us to extract two factors with a cumulative percentage variance of 63.5%. A study with Varimax rotation yielded the relative weight of each item for the two factors. Factor 1 included items 1, 3 and 4. Factor 2 included items 2, 5, 6, 7, 9 and 10; item 8 was correlated to both factors ( Table 3 ).
| F1 | F2 | |
|---|---|---|
| Pain intensity | 0.832 | 0.098 |
| Personal care | 0.402 | 0.867 |
| Lifting | 0.756 | 0.255 |
| Walking | 0.617 | 0.454 |
| Sitting | 0.384 | 0.642 |
| Standing | 0.472 | 0.539 |
| Sleeping | 0.373 | 0.612 |
| Sex life | 0.521 | 0.549 |
| Social life | 0.369 | 0.694 |
| Traveling | 0.054 | 0.835 |
Furthermore, internal consistency was assessed with Cronbach’s alpha test, it was deemed good with a Cronbach’s alpha value of 0.886 ( Table 4 ).
| Item | Correlation coefficient | P value |
|---|---|---|
| Pain | .628 | < .0005 |
| Personal care | .754 | < .0005 |
| Lifting | .711 | < .0005 |
| Walking | .716 | < .0005 |
| Sitting | .734 | < .0005 |
| Standing | .729 | < .0005 |
| Sleeping | .668 | < .0005 |
| Sex life | .717 | < .0005 |
| Social life | .755 | < .0005 |
| Traveling | .610 | < .0005 |
1.4
Discussion
This work described the different phases involved in the study of the metrological properties of the ODI translated in Arabic within a Saudi population.
1.4.1
Acceptability of the questionnaire
The time needed to complete the questionnaire was acceptable with a mean time of 3.4 minutes. In the Tunisian version, the mean time was 8.40 minutes . This could be explained in part by the fact that literary Arabic – used in the translation of the questionnaire – is closer to the Saudi dialect than the Tunisian one.
The absence of missed questions showed the good acceptability from the study participants. Compared to the original version, the Saudi version has a better item equivalence than the Tunisian one. Items 8 and 10 were not problematic for the Saudi population contrarily to the Tunisian population, even though the latter seemed more open to this type of topic . Furthermore, the Saudi population having a higher standard of living and greater annual income than the Tunisian population, with an impact on way of life where travel and getting married at a young age are more common.
1.4.2
Reproducibility
Using the Pearson correlation coefficient, the intra-observer reproducibility was calculated at 0.999 showing good reproducibility. Inter-observer reproducibility was not evaluated which constitutes one of the study’s limits.
1.4.3
Structure validity
The validity study was complicated by the fact that there is no “Gold Standard” for the functional assessment of low back pain .
Good convergent (pain VAS, the Quebec Back Pain Disability Scale and Roland–Morris Low Back Pain Disability) validity and divergent (age, weight, height and education) validity were found as expected, thus suggesting a good construct validity .
The internal consistency study using Cronbach’s alpha test yielded a value 0.866 time greater than the values found in similar studies, suggesting a good internal consistency .
The factor analysis allowed the extraction of two factors that would explain over 50% of the cumulative variance. The first focused on dynamic physical activities and the second on static activities. This result is similar to the one reported by Guermazi .
The fact that sex life was correlated to both factors can be explained by the patients’ gender, men referred to it more as a dynamic activity than women which listed it as a static activity.
1.5
Conclusion
This study evaluated the metrological qualities of the Oswestry index translated in Arabic and adapted to the Saudi population. Both the appearance validity and structure validity were good, with a similar number of items than in the original version. This study suggest that the transcultural translation in Arabic requires adaptations according to the culture of the target population even if Arabic is their common language. Further studies are required in order to study the questionnaire’s responsiveness to change.
Disclosure of interest
The authors declare that they have no conflicts of interest concerning this article.
2
Version française
2.1
Introduction
De nos jours, la lombalgie constitue un véritable problème de santé publique aussi bien dans les pays industrialisés que dans les pays en voie de développement . Le coût annuel de la prise en charge des patients lombalgiques est par exemple estimé à plus de 50 billions de dollars aux États-Unis, et à 6.1 millions de francs suisses dans la fédération helvétique . En Arabie Saoudite, la prévalence de la lombalgie n’est pas encore bien établie bien qu’elle a été estimée à 26,2 % .
C’est une affection bénigne, spontanément résolutive dans la majorité des cas . Elle touche préférentiellement le jeune adulte actif. L’examen clinique est certes important dans l’évaluation du malade, mais il ne permet pas d’évaluer le retentissement de la maladie sur le statut fonctionnel du patient .
Plusieurs échelles ont été développés pour l’évaluation fonctionnelle du patient lombalgique, dont peu d’entres elles ont été validés .
Parmi ces indices, le « Roland–Morris Disability Questionnaire » , le « Dallas Pain Questionnaire » , le « Québec Back Pain Disability Scale » , le « Waddell Disability Index » , le « Million Visual Analog Scale » , le « Low Back Outcome Score » et l’indice « Oswestry Low Back Pain Disability Questionnaire (ODI) » . Ce dernier est l’un des plus utilisé dans la littérature mondiale. Sa création remonte aux années 1980 avec des adaptations au fil des années pour aboutir à la version finale 2.1 .
Cette échelle a été validée en différentes langues dont l’arabe sur une population tunisienne . Ceci offre la possibilité de faire des études comparatives dans différentes régions du globe. Cependant, aucun indice n’a été validé en Arabie Saoudite.
L’objectif de notre travail a été d’étudier les propriétés métrologiques de la version arabe tunisienne de l’ODI sur une population saoudienne de lombalgiques.
2.2
Matériels et méthodes
2.2.1
L’indice
L’indice d’Oswestry ( Annexe A ) est un auto-questionnaire de dix items, chaque item comporte six niveaux de réponses côtés de 0 à 5. Ces items sont : la douleur, les soins personnels, le port et le déplacement des objets, les difficultés à la marche, la position assise, la position debout, les troubles du sommeil causés par la lombalgie, la vie sexuelle, la vie sociale et les voyages. Un score total est établi en pourcentage d’incapacité (score obtenu divisé par 50 puis multiplié par 100) et s’étend de 0 % (aucune incapacité) à 100 % (incapacité totale). L’interprétation de cet indice se fait en fonction des scores : de 0 à 20 % : incapacité minime ; de 20 à 40 % incapacité modérée ; de 40 à 60 % : incapacité sévère ; de 60 à 80 % lombalgie invalidante et au-delà de 80 % il s’agit de sujet grabataire, soit d’une incapacité ressentie excessive .
2.2.2
L’adaptation du questionnaire
Nous nous sommes inspirés de la version tunisienne validée . Une traduction en arabe (proche du dialectal) a été effectuée selon la méthode de traduction/contre traduction des items manquants dans la version tunisienne (items 8 et 10) . La version intermédiaire et définitive ont été soumises à la critique d’un comité d’experts composé de 4 professionnels linguistiques, 2 physiothérapeutes, et un médecin physique et de réadaptation, pour apporter les adaptations nécessaires aussi bien sur le plan linguistique que culturel.
2.2.3
Pré-test
L’échelle traduite a été testée sur un groupe de 100 personnes saines, consentantes de la population générale (pré-test) afin de vérifier l’acceptabilité du questionnaire, en évaluant la compréhension des questions et le nombre de réponses manquantes. Ces personnes proviennent de 10 régions différentes du royaume (Riyad, Assir, Bisha, Mecca, Al-Medina, Qassim, Arar, Hafr El-Baten, Dammam, Jeddah).
Vingt physiothérapeutes volontaires (10 hommes et 10 femmes) à raison de 2 par régions (un homme et une femme) étaient chargés de faire le pré-test. Le choix des régions a été fait en fonction des caractéristiques géographiques et linguistiques du royaume. Seules les personnes qui parlaient l’arabe étaient incluses dans l’étude. À la fin de cette étape, une échelle intermédiaire a été obtenue.
2.2.4
Étude de la série
2.2.4.1
Patients
Ont été inclus dans cette étude les patients âgés de 18 à 65 ans adressés au service de rééducation pour lombalgie mécanique chronique.
Les données cliniques et démographiques ont été recueillies pour tous les patients lors de la première visite. Seuls les patients stables cliniquement étaient choisis pour l’étude de la reproductibilité.
Les questions ont été énoncées mot à mot comme elles sont rédigées. L’investigateur ne pouvait pas changer les mots mais avait la possibilité de répéter les questions. Le niveau de compréhension ainsi que l’acceptabilité ont été notés pour chaque question.
2.2.5
Évaluation des propriétés métrologiques de la version finale
2.2.5.1
Faisabilité et acceptabilité
La faisabilité et l’acceptabilité de l’échelle ont été appréciées par le nombre de données manquantes pour chaque item, par la compréhension des questions posées et par le temps nécessaire pour répondre au questionnaire.
2.2.5.2
Étude de la reproductibilité
Le questionnaire a été administré à deux reprises par le même investigateur avec un intervalle de deux jours pour 50 patients. Le choix de cet intervalle a été dicté par la nécessité de la stabilité du statut clinique, d’une part, et l’absence de mémorisation des réponses, d’autre part (temps nécessaire pour remplir le questionnaire, nombre de réponses manquantes).
2.2.5.3
Étude de la validité
2.2.5.3.1
La validité d’apparence
L’étude de la validité d’apparence a été basée, d’une part, sur l’appréciation du comité d’experts et, d’autre part, sur le jugement des utilisateurs.
2.2.5.3.2
La validité de contenu
L’étude de la validité de contenu s’est appuyée sur l’appréciation du comité d’experts.
En fonction de leur expérience, les experts ont apprécié la qualité des items de l’indice en comparant l’échelle traduite à sa version originale.
2.2.5.3.3
La validité de structure
En absence de « Gold Standard », l’évaluation de la validité de structure a reposé sur l’étude de la validité de structure externe (dite de construit), qui comporte la validité convergente et divergente ainsi que l’étude de la validité de structure interne.
La validité de convergence a été évaluée en corrélant le score global de l’indice d’Oswestry avec le score de variables proche mesurant l’incapacité fonctionnelle et ou la douleur. Les variables utilisées ont été : l’EVA douleur, le score de l’indice de Roland–Morris et le score de l’indice de Québec.
La validité de divergence a été étudiée par la corrélation du score global de l’indice d’Oswestry avec des variables connues comme ayant une corrélation nulle ou minime avec la douleur ou l’incapacité fonctionnelle. Ces critères sélectionnés sont : l’âge, le poids, la taille, et le niveau d’éducation.
Une analyse factorielle suivie d’une rotation orthogonale (Varimax) a permis l’étude de la structure factorielle de l’échelle. La cohérence interne de l’indice ainsi que celle de chaque facteur extrait après l’analyse factorielle ont été étudiées par le coefficient alpha de Cronbach.
2.2.6
Analyse statistique
Le programme SPSS pour Windows (version 14) a été utilisé pour l’analyse statistique et menée avec un p < 0,05.
Les variables quantitatives ont été décrites en utilisant les moyennes, l’écart-type et les limites. Les variables qualitatives ont été décrites en utilisant des proportions et des pourcentages.
La reproductibilité a été appréciée par l’étude du coefficient de corrélation intra-classe (CCI) item par item et pour le score global. Une bonne reproductibilité était retenue si le coefficient est supérieur à 0,7 .
Les validités de convergence et de divergence ont été étudiées à l’aide du test de Kruskall–Wallis pour les variables discontinues, et à l’aide du coefficient de corrélation de Spearman pour les variables continues. Pour ce dernier, en fonction de la valeur du coefficient, selon Fermanian, les résultats ont été qualifiés d’excellents si r > 0,91, bons si 0,71 < r < 0,9, moyens si 0,51 < r < 0,7, faibles si 0,31< r < 0,5, très mauvais ou nuls si r < 0,3 .
L’analyse factorielle a été réalisée en composantes principales pour extraire les facteurs principaux. Les facteurs retenus avaient une valeur supérieure à 1. Les facteurs indépendants ont été obtenus en utilisant la méthode de rotation Varimax. La cohérence interne de chacun des facteurs retenus a été étudiée par le coefficient alpha de Crohnbach. Un coefficient supérieur à 0,7 reflète une bonne cohérence.
2.3
Résultats
2.3.1
L’échelle intermédiaire et pré-test
Pour les items 8 et 10, la technique de traduction/contre traduction a permis de réaliser des adaptations linguistiques, en privilégiant le sens plutôt que la traduction littérale.
Cette étape a donné lieu à certaines modifications linguistiques des différents items de l’échelle : les termes qui paraissaient difficiles à assimiler par les patients ont été échangés par d’autres plus simples tout en conservant le sens des questions. Les principales modifications ont été d’ordre sémantique et syntaxique.
Ainsi les termes « Awjaa » et « Wajaa », utilisés dans la version tunisienne, ont été remplacé respectivement par les termes « Aalam » et « Alam » plus proche de la culture saoudienne, ces termes étant des synonymes dans la langue arabe littérale signifiant douleur et doléances. De même, l’adjectif « lombaire » a été ajouté au terme douleur pour tous les items.
L’échelle intermédiaire de notre indice a fait l’objet d’une pré-étude et a été complétée par 100 personnes saines (50 femmes et 50 hommes) d’âge moyen 39,7 ans (min 18 ; max 65) dont 19 sont illettrées.
Ni le nombre d’items, ni les modalités de réponse n’ont été modifiés après le pré-test.
2.3.2
Données cliniques et démographiques de la série
Nous avons retenu pour l’étude finale 100 patients dont 45 % étaient de sexe féminin, l‘âge moyen était de 40,39 ± 12,70 ans, le poids moyen était de 75,64 ± 16,03 kg, la taille moyenne était de 164,96 ± 9,15 mm. Seulement 12 % étaient sans profession au moment de l’étude.
La répartition selon le niveau d’étude était comme suit : primaire : 11 ; collège : 12 ; secondaire : 24 ; universitaire : 42 ; et illettrés : 11.
2.3.3
Modifications apportées à l’échelle intermédiaire
Après étude de la série aucune modification n’a été apportée à l’échelle intermédiaire et aucun item n’a été retiré.
2.3.4
Propriétés métrologiques de l’indice
2.3.4.1
Faisabilité et acceptabilité
Le temps moyen pour remplir le questionnaire a été de 3,4 minutes (min 2 ; max 6).
L’acceptabilité a été jugé bonne pour tous les items.
2.3.4.2
La reproductibilité
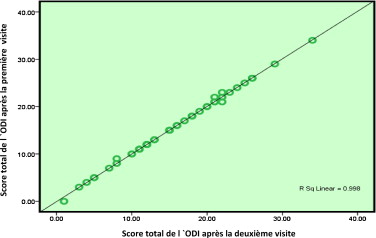
Le CCI a été de 0,999 (IC à 95 % : 0,998–0,999). La reproductibilité intra-observateurs a été jugée excellente ( Fig. 1 ). La reproductibilité item par item a montré un coefficient de corrélation allant de 0,75 a 0,99. ( Tableau 1 ).
Related posts:
 Enhancing Annalsvalue through quality
Six years of bilingual edition for The Annals of PRMare coming to an end
Pain during injections of botulinum toxin in children: Influence of the localization technique
Use of psychoactive substances in persons with spinal cord injury: A literature review
Teres major tendon tears in a professional boxer
The motor function measure to study limitation of activity in children and adults with Charcot-Marie-Tooth disease
Enhancing Annalsvalue through quality
Six years of bilingual edition for The Annals of PRMare coming to an end
Pain during injections of botulinum toxin in children: Influence of the localization technique
Use of psychoactive substances in persons with spinal cord injury: A literature review
Teres major tendon tears in a professional boxer
The motor function measure to study limitation of activity in children and adults with Charcot-Marie-Tooth disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


