FIGURE 6.1 Lateral aspect of right shoulder (red arrow indicates path of the needle). (From Tank PW, Gest TR. Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins, 2009.)
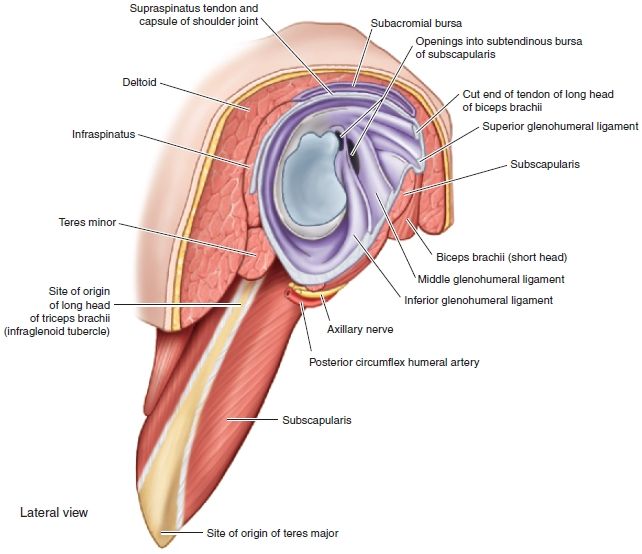
FIGURE 6.2 Interior of right shoulder. (From Tank PW, Gest TR. Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins, 2009.)
PATIENT POSITION
- Sitting on the examination table.
- The patient’s hands are folded in his or her lap with fingers interlaced.
- This allows consistency of positioning of the shoulder so that the landmarks do not change from the time that they are identified and marked until the time of injection.
LANDMARKS
1. With the patient seated on the examination table, the clinician stands lateral and posterior to the affected shoulder.
2. Find the lateral edge of the acromion, and mark it with an ink pen.
3. Palpate the posterior edge of the acromion and mark that.
4. Having identified the posterior lateral corner of the acromion, drop a vertical line down from that point and mark a spot 2 cm below the posterior lateral corner.
5. At that site, press firmly with the retracted tip of a ballpoint pen. This indention represents the entry point for the needle.
6. Next, identify the target site by placing the index finger of your nondominant hand over the superior aspect of the acromion posterior to the acromioclavicular (AC) joint. This will be the target for the tip of the needle (Fig. 6.3). If your index finger is at the target site—on top of the acromion—it will be protected from accidental needlestick.
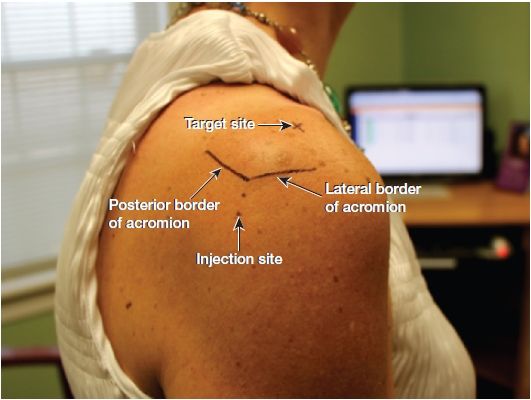
FIGURE 6.3 Right shoulder injection landmarks.
7. After the landmarks are identified, the patient should not move the shoulder or arm.
ANESTHESIA
- Tactile skin distraction is administered by firmly stroking the skin outside of the injection point as the needle is quickly introduced into the skin. Topical vapocoolant spray or injection of a local anesthetic is unnecessary in almost all patients.
EQUIPMENT
- 5-mL syringe
- 25-gauge, 2-in. needle (Consider a 3½ in., 25-gauge needle in large individuals.)
- 3 mL of 1% lidocaine without epinephrine
- 1 mL of the steroid solution (40 mg of triamcinolone acetonide)
- One alcohol prep pad
- Two povidone–iodine prep pads
- Sterile gauze pads
- Sterile adhesive bandage
TECHNIQUE
1. Prep the insertion site with alcohol followed by the povidone–iodine pads.
2. Position the needle and syringe at about a 30-degree angle to the skin with the needle tip directed cephalad toward the acromion.
3. Using the no-touch technique, introduce the needle at the insertion site (Fig. 6.4).

FIGURE 6.4 Right shoulder subacromial space injection.




