Triceps Tendon Ruptures
Andrea Celli
DEFINITION
Elbow extension against gravity or resistance may be difficult or impossible when the distal triceps tendon is ruptured or avulsed from the olecranon insertion.
Complete ruptures of all three heads tendon insertion (long, lateral, and medial heads) generally require surgical treatment.
Partial lesions are functionally well tolerated in patients with low functional demand.
ANATOMY
Origin
The triceps brachii (FIG 1) has three heads:
The long head arises from the infraglenoid tubercle of the scapula.
The lateral head has a linear attachment from the upper margin of the radial grove of the humerus.
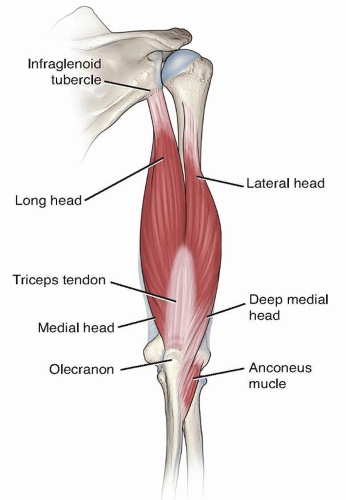
FIG 1 • Triceps brachii anatomy.
The medial head originates below the lateral margin of the radial groove that contains the radial nerve. Its insertion covers the entire rear surface of the lower part of the humerus.
Insertion
In the distal third of the posterior aspect of the arm, the lateral head joins with the long head to form the superficial tendinous part of the insertion on the posterior surface of the olecranon. The medial head (deep part of the triceps) inserts through muscular and tendinous fibers directly onto the olecranon.
The superficial tendon forms two components as it approaches its insertion area (FIG 2):
A lateral part that is more expansive and relatively thin and in continuity with anconeus muscle and fascia
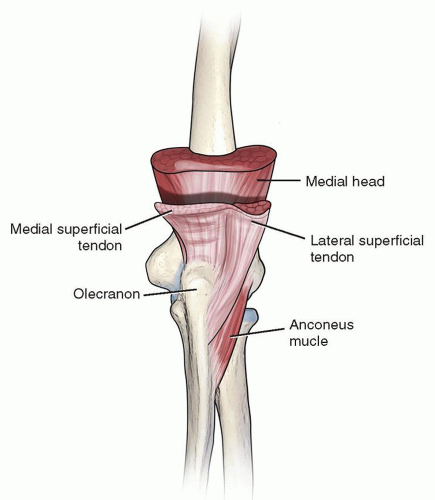
FIG 2 • The distal triceps tendon insertion (superficial and deep components): The lateral aspect of the tendon is more expansive, relatively thin, and in continuity with anconeus muscle and fascia. The medial part is thicker than the lateral aspect and forms the proper triceps tendon. It inserts directly onto olecranon.
A medial part of the tendon that is thicker than the lateral aspect and forms the proper triceps tendon and inserts directly onto olecranon
In some cases, a well-defined interval is located between the lateral triceps expansion and medial triceps tendon just proximal to the olecranon. This interval is located along the crest of the ulna and is well known as triceps decussation.
The deep tendon is covered by a thin layer of muscle fibers both medially and laterally.
The deep medial head of the triceps shows a broad and flat tendon centrally and laterally, whereas medially is a narrow thickened tendon.22
Medially, the superficial and deep tendons are confluent and form the proper triceps tendon that insert into the medial olecranon footprint.
Magnetic resonance imaging (MRI) often demonstrates a bipartite insertion between the deep and superficial tendon of the triceps into the olecranon7 (FIG 3).
Olecranon Footprint
The mean medial to lateral width of the insertion area is about 20 mm and the mean proximal to distal length22 is about 13 mm.
The mean distance from the olecranon tip to the most proximal aspect of the medial head insertion4,22 is between 14.8 and 16 mm.
The mean width (medial to lateral distance) of the medial head footprint is 16 mm and the mean thickness is 4 mm.
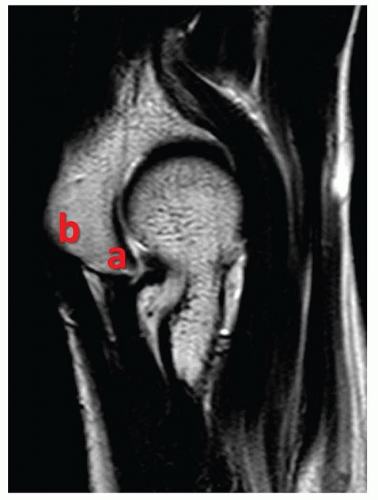
FIG 3 • The MRI demonstrating a bipartite insertion between the deep (a) and superficial (b) components of the triceps tendon into the olecranon.
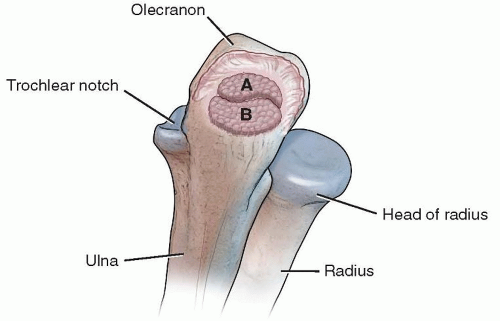
FIG 4 • The mean width (A) of the medial head footprint is about 16 mm and the mean thickness is 4 mm. The mean width of the common superficial tendon footprint is 19 mm and the mean thickness is 8 mm (B).
The mean width of the common superficial tendon footprint is 19 mm and the mean thickness4 is 8 mm.
Understanding the anatomy of the triceps tendon is the key to good outcomes following posttraumatic triceps repair or triceps reinsertion after deep surgical exposure.
PATHOGENESIS
Triceps tendon injuries are probably one of the rarest tendon injuries in the body. There is a male predominance (3:1, male to female) with a wide range of age in which it can occur.56
Triceps tendon ruptures can be simply classified into one of four groups:
Traumatic lesion (most common)
Spontaneous rupture
Overuse injury
Following total elbow arthroplasty
Traumatic Lesions
Triceps tendon ruptures most commonly occur acutely when a patient falls on an outstretched hand with the elbow in some flexion and a forced load is applied to the contracting triceps. Traumatic tears can occur at several different anatomic regions, but they are most commonly observed at the insertion of the tendon such as an olecranon avulsion. More rarely, they can occur at the musculotendinous junction or within the muscle belly.3,5,39
The traumatic distal tendon lesions can be partial or total5,23 and are often isolated. Associated lesions of the radial head,30,31 the medial collateral ligament (MCL),24,32,49 and the capitellum57 have been described.
Partial traumatic tendo-osseous avulsions with one small fragment of bone visible proximal to the olecranon (flake sign) often occur associated with the radial head fractures31 or simultaneous radial head and MCL-associated injuries.57
The combination of a triceps avulsion, radial head fractures, and MCL rupture were reported by Yoon et al57 as triad injury.
Spontaneous Ruptures
Triceps injury can occur spontaneously due to attrition conditions if the tendon integrity is compromised. Loss of integrity can be caused by the following:
Rheumatoid arthritis
Chronic renal failure
Endocrine disorders
Metabolic bone diseases
Steroid use (local or systemic corticosteroids or anabolic steroids)18
Tenosynovial pathologic tissue proliferation in the tendon combined with low local blood supply and mechanical attrition results in rupture of the tendon.
Overuse Injuries
The cumulative submaximal loading of the tissue is referred to as overuse injuries, and complete rupture often occurs through abnormal tendon with intrinsic pathologic disorders.19
A classification of progressive Achilles tendon disorders46 can be useful to understand the structural manifestations of triceps tendon overuse injury.
Peritendinitis
Tendinosis with or without peritendinitis
Partial rupture
Total rupture
Triceps tendinosis during sporting activities is not infrequent. In cases of chronic tendon pain, the pathologic lesion is typical of a degenerative process with areas of marked degeneration and lack of local vascular supply.2 These characteristic changes, especially if associated with a repetitive use of local corticosteroids, predispose to triceps tendon rupture, possibly by decreasing the tendon tensile strength.
Surgical treatment is recommended in chronic tendinosis when clinical and MRI assessments detect partial rupture of the tendon.
Following Total Elbow Arthroplasty
Failure of triceps reattachment can be seen following surgical treatment in which a triceps takedown is performed.
When the total elbow arthroplasty is performed, the surgical triceps takedown or slide is usually well tolerated, but some patients have an unsuccessful postsurgical attenuation or ruptures of the triceps reattachment.
At the Mayo Clinic, this complication occurred in 16 elbows following 887 total elbow arthroplasties, about 2% of the procedures.10
Predisposing factors are inflammatory arthropathies with poor tissue quality.
The triceps weakening is a frequent and a well-recognized problem following the total elbow arthroplasty.
The causes of the triceps weakness or rupture following arthroplasty may be related to the following:
Changes of the triceps moment arm which is a function of location of the axis of the prosthetic joint.14 The offset of the triceps tendon decreases (reducing the strength of the muscle) when the prosthesis design is not anatomic. Insufficient reinsertion related to poor quality of tendon tissue or tendon devascularization during the approach.
Aggressive rehabilitation program during the postoperative period with active exercises that can attenuate or detach the triceps reinsertion
PATIENT HISTORY AND PHYSICAL FINDINGS
In patients with suspected rupture of triceps tendon, the physician should gather a precise history including:
Age, dominant arm
Presence of preexisting pain from overuse injuries44
Repetitive use of local corticosteroids or systemic anabolic steroids12
Previous elbow surgery
The patient most commonly describes a sudden pain in the posterior aspect of the elbow after a history of direct blow or fall on outstretched hand.16,17,29,38 The usual mechanism of injury is a forceful sudden flexion of extended elbow.48,49,50
Laceration and open injuries with or without elbow fracture-dislocation can also cause distal triceps rupture.27
In general, the triceps lesions is characterized by the following:
Tenderness and a palpable defect in the tendon that can be seen proximal to the olecranon
Swelling, ecchymosis, and body habitus can obscure the tendon defect in the acute stage. Once swelling subsides, most patients demonstrate a palpable gap in the tendon.
A partial rupture of the medial head is frequently undiagnosed. The diagnosis can be difficult, but care should be taken when evaluating radiographs to assess for the presence of the flake sign.
The clinical findings of the triceps insufficiency following total elbow arthroplasty are as follows10,11:
A change in the posterior contour of the elbow with visual and palpable prominence of the implant
The presence of olecranon bursitis
Atrophy of the triceps muscle
Proximal retraction or lateral subluxation of the extensor mechanism
The most universal physical finding with a triceps rupture is the inability to extend the arm against gravity (FIG 5).
A tear can be seen and palpated in the tendon during attempts at resisted extension (FIG 6A,B).
Discerning between partial or complete ruptures can be a diagnostic challenge. The test to evaluate the triceps function against gravity and resistance is performed by the physician
with the patient in the prone position with the elbow flexed to 90 degrees, the upper arm supported on the table, and the forearm hanging free (FIG 7).

FIG 5 • The triceps extension tests can be performed observing the ability of the patient to extend the elbow over his or her head, against gravity.

FIG 6 • A. The clinical findings of the triceps insufficiency are a change in the posterior contour of the elbow with visual and palpable prominence of bone. B. A tear can often be palpated in the triceps tendon.
A partial tendon lesion is manifested by weakness and ability to actively extend the elbow against the gravity but not against resistance. This finding is likely secondary to an intact lateral expansion or a compensating anconeus muscle.
A total tendon tear is manifested by loss of extension strength against gravity, and active elbow extension is impossible. Viegas51 described a provocative test similar to the Thompson test that can be employed in diagnosing triceps tendon rupture. With the patient in the prone position and the forearm hanging over the side of the table, the physician squeezes the triceps muscle belly. Slight elbow extension is indicative of a partial tear, whereas no motion signals a complete rupture (FIG 8).
We have defined a test for triceps rupture called the fall down triceps test. This test assesses the inability of the patient to keep the forearm in maximum extension against gravity. The patient stands up with the shoulder at 90 degrees of abduction and internal rotation, the examiner stays behind and keeps the forearm in full passive extension. If the forearm falls when the examiner releases it, there is a triceps tendon rupture (FIG 9).
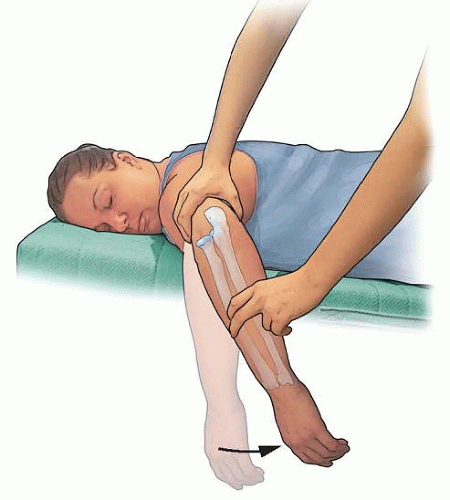 FIG 7 • Elbow extension can be evaluated with the patient in the prone position with the elbow flexed to 90 degrees, the upper arm supported on the table, and the forearm hanging free.
Related posts: Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
 Fragment-Specific Fixation of Distal Radius Fractures Fragment-Specific Fixation of Distal Radius Fractures
 Arthroscopic and Open Triangular Fibrocartilage Complex Repair Arthroscopic and Open Triangular Fibrocartilage Complex Repair
 Synovectomy of the Elbow Synovectomy of the Elbow
 Surgical Treatment of Septic Arthritis in the Hand and Wrist Surgical Treatment of Septic Arthritis in the Hand and Wrist
 The Use of Free Vascularized Fibular Grafts for Reconstruction of Segmental Bone Defects The Use of Free Vascularized Fibular Grafts for Reconstruction of Segmental Bone Defects
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|